
Why I don't do vaginal exams ~ Wisdom from a Traditional Birth Companion

I was talking with my new client about what would likely happen when I arrived at her home when she was in labour. We talked about sanitation measures, spending time in the kitchen, setting up the pool, and where I could take a nap if she needed some privacy. I said I would not be doing any vaginal exams as I think they’re rude, and she wept with relief.
I specialise in trauma and the majority of my clients are refugees from the medical system, running from ritual abuse and routines that protect the industry. They want someone to mentor them through to a healthy birth without the traps and trappings of the industry that removed their choice, and violated their autonomy and their dignity.
We won’t go into the history of obstetrics that began with the burning of witches (midwives and healers), the rise of the man-midwife, the development of lying-in hospitals, and eventually the wholesale co-opting and medicalisation of birth. Suffice it to say that obstetrics and hospitalisation didn’t “save” women and babies (1). It created untold harm and mortality until they learned better infection control and saner behaviours. Today, it’s still leaving a trail of destruction as about 1/3 of their clients are traumatised (2,3,4) and about 1 in 8 enter parenthood with postpartum post-traumatic stress disorder (5,6,7). Suicide is a leading cause of maternal death in the first year and is highly correlated to trauma (8,9,10,11,12,13,14,15,16). It’s an industry out of control with unjustifiable caesarean rates, dangerous inductions for spurious reasons, and wholesale overuse of medications and interventions.
What women didn’t notice in this process of medicalisation and co-opting of their physiology for profit is that the medical industry took ownership of their vaginas once they became pregnant. Pregnancy transfers ownership of the vagina from the woman to the industry. Midwifery and obstetrical regulations stipulate that inserting an instrument, hand, or finger beyond the labia majora is a restricted practice sanctioned by legislation (17). To test this, see how long it takes for someone in the industry to file a Cease and Desist or start a campaign of persecution for the purpose of prosecution if they catch wind of anyone but one of their own sticking their fingers up there. No one but an insider sticks their fingers into their territory. It doesn’t matter who the mother gives her permission and consent to - it must be a member of the priesthood of modern medicine.
Of course, in their benevolence, they’re generally quite accommodating where partners are concerned, because most partners are male and obstetrics is exceedingly misogynistic. They value the needs and the pleasures of the D.
As a traditional birth attendant, I don’t do vaginal exams. For one thing, it’s considered a restricted practice for just the medical pundits and not doing them with my clients keeps the industry players somewhat placated knowing I’m not intruding into their turf. But the real reason is because I think they’re completely unnecessary and wouldn’t do them even if the medical folks begged me to under the guise that it would make birth safer.
To better understand the offence of the routine vaginal exam, we have to go back in time to when the male-midwife moved into the sanctity of women-centred birth and the domain of the midwife. It was profitable. And they convinced the public that they would provide a superior service based on the cultural belief of the time that women were disadvantaged by an inferior intellect and a predilection for sorcery (18,19). They also brought with them the medical perspective that women were an error of nature and that the world, and thus its inhabitants, were but a machine that could be best understood by coming to know its parts in isolation of the whole.
And so began dissection, mechanisation, and reducing birthing women to their parts. She became a womb expelling a foetus through a vagina. Think of today’s obstetrical “power, passenger, passage” perspective on how birth unfolds. Not much has changed in 400 years.
By sticking their fingers up there, they discovered that the cervix opens to expel the foetus. Oh, happy day! From the morgue to the birth suite, physician fingers were poking everything. Throughout the early and mid 1800’s, the infection rate in some hospitals soared as high as 60% from the mysterious childbed fever, with death rates as high as 1 in 4 (20). Nothing the doctors did was contributing to this mystery as physicians were gentlemen and gentlemen didn’t carry germs (21). And once they did accept that their filthy practices were killing women, rather than abandon the idiocy of penetrating their patients in labour, they eventually figured out how to make it less dangerous.
The practice of obstetrics has always been highly resistant to change and common sense. After all, they’ve had 400 years to figure things out and women are still birthing on their backs!
Once it was discovered that the cervix dilates as part of the labouring process, the medical industry has been fixated on that bit of tissue and made it the focus of their entire assembly line drive-through everyone-gets-what’s-on-the-menu service. That bit of tissue determines how the ward allocates services, whether the client will be permitted to stay, and how long she’ll be allowed to use their services before the next client needs the bed.
Thanks to Dr. Emanuel Friedman, who examined the cervices of 500 sedated first-time mothers in the 1950’s and plotted their dilation on a graph and matched it to the time of their birth – we now have the infamous Friedman’s Curve and the partogram.

© Evidence Based Birth
The partogram is a graph that plots cervical dilation and descent of the foetal head against a time-line. When the graph indicates that progress is slower than is allowable according to the particular chart chosen by their institution, then the practitioner is called upon to administer various interventions to speed things up to keep the labour progressing well, aka, profitably. Should these acceleration measures fail to produce a baby in a timely manner or cause foetal distress, then a caesarean section is the solution. “Failure to progress”, and the accompanying foetal distress that is often a consequence of those acceleration measures, are the leading causes of a primary caesarean (22).

Obstetrical partogram
In addition to clearing the bed for the next client, obstetrics has another reason for expediting labour. The more vaginal exams a woman receives, the greater the likelihood she’ll develop a uterine infection (23). So, once they start the poking, they need to get the baby out before their prodding adds another problem for them to solve.
In the absence of a medical situation, routine vaginal exams in labour are for the purpose of charting in order to maintain a medicalised standard of modern technocratic birth.
A labouring client will not be admitted to a hospital without a vaginal exam to determine if her dilation is far enough along for their services (unless she’s clearly pushing). And this isn’t necessarily a bad thing. Early admission to the hospital results in more interventions and more caesareans than later admission (24). This is a business and time is money.
A regulated midwife attending a homebirth will likewise perform a vaginal exam upon arrival at the client’s home to determine if the client is far enough along to warrant their limited resources and time by staying and beginning the partogram or leaving and waiting to be called back later. They must also follow the rules of the hospital at which they have privileges or their regulatory agency and transport for augmentation/acceleration if the partogram shows a significant variation.
All of this is predicated on the outdated and obsolete notion that women are machines and birth is a linear process. The only thing a vaginal exam reveals is where the cervix is sitting at that particular moment and how it’s interpreted by that particular practitioner. Women are not machines and birth is not linear. Just like any mammal, birth can be slowed, stopped, or sabotaged by an unfavourable environment or reckless attendants. I’ve said for years that it’s so easy to sabotage a good birth, it’s embarrassing.
“Years ago, I was with a first-time mother planning a family-centred homebirth. She was on the clock and had a deadline. At 42 weeks gestation, she had until midnight that night to produce a baby in order to have a midwife-attended homebirth. After that, she was expected to report to the hospital for a chemical induction. As her contractions built throughout the day, her preferred midwife arrived and labour was progressing well. She was enjoying the process and the camaraderie of her sisters-in-birth. Eventually, one of the vaginal exams revealed a cervical dilation of 8 cm, indicating it was time to call in the 2nd midwife. Only, it was a midwife that had routinely upset the mother throughout pregnancy with requests for various tests and talk of all the dangers of declining routine testing. Upon learning this midwife was coming to the birth, labour slowed.
Soon enough, the 2nd midwife arrived and assumed authority over the birth process and insisted on repeated vaginal exams for the purpose of staying within the parameters of the partogram. Her vaginal exams were excruciating, no doubt because she was trying to administer a non-consenting membrane stripping as an intervention to address the slowed and almost non-existent contractions. Eventually, an exam revealed a dilation of only 6 cm. After several more hours of “torture” (according to this mother’s recount) to keep labour going rather than just leaving the mother to rest and accepting that this labour had been hijacked and needed time to regroup and restart, dilation regressed to 4 cm and the mother eventually ended up acquiescing to a hospital transfer, and experienced an all-the-bells-and-whistles birth, trauma, and postpartum PTSD.
This mother’s subsequent birth a couple of years later didn’t include inviting midwives and unfolded as it was meant to. After a day of productive and progressing labour that was clearly evident without sticking fingers up her vagina, she eventually got tired and labour slowed and stopped. She went to bed and I went home. When she woke up, labour resumed and a baby emerged swiftly and joyously. As it turns out, for her, she has a baby after a good sleep with people she trusts.”
What about the routine vaginal exams in late pregnancy? Glad you asked!
Since they don’t have good predictive value, meaning they won’t diagnose when labour will begin, how long it will take, or whether the woman’s pelvis will accommodate that particular baby prior to labour, they have 2 functions.
The first is to plan and initiate your induction.
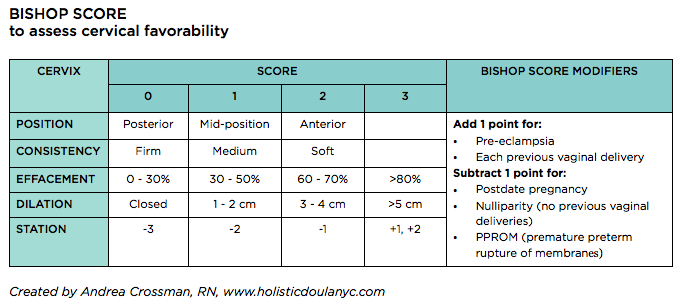
A cervical exam provides information that is measured against a Bishop Score. A Bishop Score provides a predictive assessment on whether an induction is likely to result in a vaginal birth or is more likely to result in a caesarean for “failure to progress”. A cervix that scores higher is more likely to respond to an induction whereas a lower score indicates a less favourable outcome (25). Further, a vaginal exam allows the practitioner to begin the induction process with a membrane stripping/stretch-and-sweep.
The second purpose for routine vaginal exams in pregnancy is to build in sexual submission. It reaffirms the power dynamic where someone who is not the woman’s intimate sexual partner is allowed to penetrate her genitals at will. It makes their job much simpler once she’s is in labour. She has been trained to accept this violation.
A vaginal exam during labour might rarely be indicated when there is a problem that requires more information. A vaginal exam can help determine if there’s a possible cord prolapse requiring immediate medical attention, or can asses the position and descent of the baby to help suggest strategies to encourage the baby to move into a better position. However, when a labour is spontaneous, meaning it hasn’t been induced by any mechanical, chemical, or “natural” means, the labour isn’t augmented with artificial rupture of membranes or synthetic oxytocin, and the labouring woman is untethered and free to move as her body indicates, complications are far less likely.
Throughout my 35 years in supporting birthing families, I can say that babies do indeed come safely and spontaneously out of vaginas when there’s no one sticking their fingers up there. And they tend to come more quickly. Routine vaginal exams don’t contribute to the safety of the mother/baby. However, they do add to the safety of the practitioner who is tasked with placating the technocratic gods who demand they follow protocols and keep the wheels of the business running on track.
My reasons for not doing vaginal exams, even if the the technocratic gods gave their blessing, include:
They’re rude
They’re unnecessary
They shift the locus of power from the birthing woman to the person with the gloves
They introduce the potential for infection
They interrupt labour and can sabotage a good birth
They often hurt
They can traumatise the cervix
They can traumatise the mother
They can impact the experience of the baby
There are so many simpler ways to determine how labour is progressing
I don’t practice medicine or midwifery or engage in its absurdities
I really am not that interested in other people’s vaginas
Let’s talk about when labour does veer from a normal physiological process.
When the power dynamic places the labouring and birthing mother in charge of the experience, it actually becomes a safer and simpler process. She is the one who is experiencing the labour and birth and is the one relaying information. Only she is in direct communication with her baby. She is the one who knows when labour has exceeded her resources and she needs medical help, pharmacologic pain relief, or the reassurance of the technocratic model.
Of course, not all births unfold simply. However, my experience over these many years is that when women are not expected to submit to exams for the purpose of charting and the subsequent limitations imposed by those charts, birth unfolds a lot more simply far more often.
Much love,
Mother Billie ❤️
Endnotes
Tew, Marjorie. Safer childbirth?: a critical history of maternity care. (2013). Springer.
Garthus-Niegel, S., von Soest, T., Vollrath, M. E., & Eberhard-Gran, M. (2013). The impact of subjective birth experiences on post-traumatic stress symptoms: a longitudinal study. Archives of women's mental health, 16(1), 1-10.
Creedy, D. K., Shochet, I. M., & Horsfall, J. (2000). Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth, 27(2), 104-111.
Schwab, W., Marth, C., & Bergant, A. M. (2012). Post-traumatic stress disorder post partum. Geburtshilfe und Frauenheilkunde, 72(01), 56-63.
Montmasson, H., Bertrand, P., Perrotin, F., & El-Hage, W. (2012). Predictors of postpartum post-traumatic stress disorder in primiparous mothers. Journal de gynecologie, obstetrique et biologie de la reproduction, 41(6), 553-560.
Beck, C. T., Gable, R. K., Sakala, C., & Declercq, E. R. (2011). Posttraumatic stress disorder in new mothers: Results from a two‐stage US National Survey. Birth, 38(3), 216-227.
Shaban, Z., Dolatian, M., Shams, J., Alavi-Majd, H., Mahmoodi, Z., & Sajjadi, H. (2013). Post-traumatic stress disorder (PTSD) following childbirth: prevalence and contributing factors. Iranian Red Crescent Medical Journal, 15(3), 177-182.
Oates, M. (2003). Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. British medical bulletin, 67(1), 219-229.
Oates, M. (2003). Suicide: the leading cause of maternal death. The British Journal of Psychiatry, 183(4), 279-281.
Cantwell, R., Clutton-Brock, T., Cooper, G., Dawson, A., Drife, J., Garrod, D., Harper, A., Hulbert, D., Lucas, S., McClure, J. and Millward-Sadler, H. (2011). Saving Mothers' Lives: Reviewing maternal deaths to make motherhood safer: 2006-2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG: an international journal of obstetrics and gynaecology, 118, 1-203.
Austin, M. P., Kildea, S., & Sullivan, E. (2007). Maternal mortality and psychiatric morbidity in the perinatal period: challenges and opportunities for prevention in the Australian setting. Medical Journal of Australia, 186(7), 364-367
Palladino, C. L., Singh, V., Campbell, J., Flynn, H., & Gold, K. (2011). Homicide and suicide during the perinatal period: findings from the National Violent Death Reporting System. Obstetrics and gynecology, 118(5), 1056.
Grigoriadis, S., Wilton, A.S., Kurdyak, P.A., Rhodes, A.E., VonderPorten, E.H., Levitt, A., Cheung, A. and Vigod, S.N. (2017). Perinatal suicide in Ontario, Canada: a 15-year population-based study. Cmaj, 189(34), E1085-E1092.
CEMD (Confidential Enquiries into Maternal Deaths) (2001) Why Mothers Die 1997–1999. London: Royal College of Obstetricians and Gynaecologists.
Sareen, J., Cox, B. J., Stein, M. B., Afifi, T. O., Fleet, C., & Asmundson, G. J. (2007). Physical and mental comorbidity, disability, and suicidal behavior associated with posttraumatic stress disorder in a large community sample. Psychosomatic medicine, 69(3), 242-248.
Hudenko, William, Homaifar, Beeta, and Wortzel, Hal. (July 2016). The Relationship Between PTSD and Suicide. PTSD: National Center for PTSD, U.S. Department of Veterans Affair.
Act, Ontario Midwifery. "SO 1991, c. 31." (1991).
Smith Adams, K. L. (1988). From 'the help of grave and modest women' to 'the care of men of sense': the transition from female midwifery to male obstetrics in early modern England. (Master’s thesis, Portland State University.
Burrows, E. G., & Wallace, M. (1998). Gotham: a history of New York City to 1898. Oxford University Press.
Semmelweis, I. (1983). Etiology, concept, and prophylaxis of childbed fever. Carter KC, ed. Madison, WI.
Halberg, F., Smith, H. N., Cornélissen, G., Delmore, P., Schwartzkopff, O., & International BIOCOS Group. (2000). Hurdles to asepsis, universal literacy and chronobiology-all to be overcome. Neuroendocrinology Letters, 21(2), 145-160.
Caughey, A. B., Cahill, A. G., Guise, J. M., Rouse, D. J., & American College of Obstetricians and Gynecologists. (2014). Safe prevention of the primary cesarean delivery. American journal of obstetrics and gynecology, 210(3), 179-193.
Curtin, W. M., Katzman, P. J., Florescue, H., Metlay, L. A., & Ural, S. H. (2015). Intrapartum fever, epidural analgesia and histologic chorioamnionitis. Journal of Perinatology, 35(6), 396-400.
Kauffman, E., Souter, V. L., Katon, J. G., & Sitcov, K. (2016). Cervical dilation on admission in term spontaneous labor and maternal and newborn outcomes. Obstetrics & Gynecology, 127(3), 481-488.
Vrouenraets, F. P., Roumen, F. J., Dehing, C. J., Van den Akker, E. S., Aarts, M. J., & Scheve, E. J. (2005). Bishop score and risk of cesarean delivery after induction of labor in nulliparous women. Obstetrics & Gynecology, 105(4), 690-697.