
Birth Hijacked – The Ritual Membrane Sweep
Buckle up. Here we go again!

©Hanna-Barbera
I’ve written about many topics over the years but nothing has ever generated as much discussion, opposition, and vitriol as challenging the cherished routine membrane sweep/stripping, aka stretch-and-sweep.
A few years ago, I wrote a post about how I’d like to see the routine, prior-to-40-weeks, without-medical-indication membrane sweep banned from obstetrical and midwifery practice. I talked about its risks and the fact that the clients I worked with called it a sexual assault when done without consent
The post went viral and I received hate messages and emails from around the world defending this procedure. In general, the sentiment was that I should most definitely be having sexual relations with myself, after which, I should be locked up and forever silenced. I also heard from hundreds of women whose births were ruined by days of painful, non-progressing contractions triggered by a membrane sweep that ended up in a fully medicalised all-the-interventions arrival for their baby that they didn’t want. And horrifically, even more hundreds wrote to share their stories of non-consenting, painful, and violating membrane sweeping when there was no reason for it, aside from the care provider’s decision that they had agency over their patient’s vagina and could do what they wanted when they wanted.
That particular post was prompted by a brief encounter with a new mother. Her baby was little and we got talking. She told me how she went to her usual prenatal visit at 36 weeks and the doctor said it was time for a vaginal check to see how things were coming along. She thought that was an ok idea and stripped accordingly, lay down on the examining table and put her feet in the stirrups. However, rather than a simple vaginal exam, she experienced excruciating pain that had her crawling up the table trying to escape that probing hand. The doctor removed her bloodied glove and when this woman asked why she was bleeding, the doctor responded, “That should get things going”. This mother had experienced a non-consenting, unplanned, and unknowing stretch-and-sweep to start labour before she or the baby were ready. She went home bleeding and cramping and within a few days went into labour and birthed a baby that was not ready to breathe. The baby spent 3 days in the NICU and she was devastated. Her birth was hijacked by a damnable routine from someone who should have known better or at least given a damn.
Yes, that was obstetrical violence. However, the routine of membrane sweeping for the mere reason that the client is at term is a deeply embedded ritual in obstetrics and mimicked by some midwives. I don’t think there is one other procedure that so callously turns a normally progressing pregnancy into a pathological event than this heinous routine.
So what is it about membrane sweeping that is so cherished that challenging it generates death threats?
Routines are habits that help organise our days
Let’s begin with some clarity on what I’m challenging.
First and foremost, I am not challenging the right for a pregnant person to choose a membrane sweep as a means of expediting labour. I fully support an individual’s right and autonomy to choose what is best for them.
Secondly, I am not challenging this as a tool for expediting labour when there is a medical indication.
I am challenging the ROUTINE of membrane sweeping that is done by some care providers as part of their normal and usual prenatal “package”, without any hint that there is a reason to expedite the birth of the baby due to an emerging medical condition.
At your cervix, ma’am

Let’s take a tour of the cervix. The cervix is a narrow passage that sits at the lower end of the uterus extending into the vagina. The cervix changes throughout the menstrual cycle and serves an important function in fertility. During ovulation, the cervix produces sperm-friendly mucus and becomes softer and more open to facilitate sperm reaching the ovum. When not ovulating, it produces sperm-unfriendly mucus and makes it more difficult for sperm to pass through to the uterus.
In pregnancy, the cervix fills with mucus, which creates a barrier to help prevent infection from passing through to the uterus. The cervix remains closed and rigid (like the tip of your nose) and is about 3-5 cm. long.
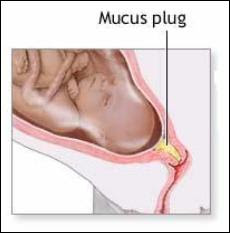
At term, in preparation for birth, the cervix will soften (like the inside of your cheek) due to the action of various hormones. The cervix is comprised of about 5-10% smooth muscle cells, which ensures it will stay closed and rigid throughout pregnancy. In preparation for labour, these muscle cells experience a programmed cellular death, which allows for the cervix to open (Leppert, 1995). The cervix will develop more oxytocin and prostaglandin receptors to help with the dilation process (Buckley, 2015). Prostaglandins, which are found abundantly in semen, ripens the cervix, digests the mucus plug, and promotes softening and shortening of the cervix.
Medical providers tend to give a great deal of attention to the cervix both prior to labour and in labour. It can provide some information that the medical folks find useful.
At term (around 40 weeks), the cervix can be felt to determine if it is ripening. Ripening means that the cervix is becoming softer, shorter, and is moving its position slightly forward. If so, it means that normal end-of-pregnancy hormones are doing their job. If not, it means that normal end-of-pregnancy hormones are doing their job, but they just haven’t gotten around to softening and shortening the cervix at the moment that a gloved hand is probing it.
This information is useful for planning an induction. A cervix that is shorter than 1.5 cm. is more predictive of spontaneous labour within the next 7-10 days than a longer cervix (Rao, Celik, Poggi, Poon, & Nicolaides, 2008). And a cervix that scores higher on the Bishop score is more predictive of an induction resulting in a vaginal birth rather than surgery (usually called “failure to progress”) (King, Pilliod, & Little, 2010). So that end-of pregnancy vaginal exam is about gathering information to plan your induction.
The other possibility for these routine (without medical indication) vaginal examinations in a healthy pregnancy is to develop submission and compliance in the client as she subjugates herself to the clinician by having her genitals penetrated by someone who is not her intimate partner.
Not too long ago, I was working with a postpartum client who was recovering from her birth experience. As a survivor of sexual assault she did not want anyone penetrating her genitals when she was labouring and giving birth and repeatedly told her midwife this. However, her midwife felt it was best for her to submit to vaginal exams in pregnancy to “get used to” them before she was in labour. Apparently, it never occurred to either of them that vaginal exams are optional and largely unnecessary for birthing a baby. In this case, the prenatal vaginal exams were for the purpose of building in submission and compliance so that the care providers could exercise agency over her body in labour.
Inductions: getting the baby out before it’s ready
An induction starts labour artificially before optimal hormonal physiology has prepared the baby and the mother for spontaneous birth. About 1 in 4 births begin by induction (BORN, 2013; Osterman & Martin, 2014). Although, there has been a slight decrease in inductions in recent years as fewer early-term inductions, meaning prior to 39 weeks, are performed. This has allowed more mothers to go into spontaneous labour without any additional adverse outcomes (Osterman & Martin, 2014). The cervix is one small part of the whole physiological process and since it can be reached easily by probing hands, it can provide a bit of information on whether an induction is likely to lead to a vaginal birth or is more likely to result in caesarean surgery.
There are lots of ways to artificially start labour before the mother or baby are ready. There are the so-called “natural” inductions:
Acupuncture and acupressure
Herbs and Homeopathy
Castor oil
Massage
Nipple stimulation
There are chemical inductions, which the literature calls “formal” inductions, as they require medical supervision:
Cervical ripening with prostaglandins
Intravenous synthetic oxytocin
And we have mechanical inductions, which also generally require medical supervision:
Artificial rupture of membranes aka “breaking the water”
Cervical ripening with a balloon catheter
Manual membrane sweeping/stripping, “stretch and sweep”
Ideally, an induction should only be suggested when the risks of staying pregnant outweigh the long and short-term risks of an induction. Depending on the method of induction those risks can include preterm birth, breathing problems in the baby, infection in the mother or baby, uterine hyper-stimulation, uterine rupture, fetal distress, breastfeeding failure, and rarely, death of either the mother or the baby.
Unfortunately, most inductions are done where the research affirms that the risks of an induction outweigh the risks of staying pregnant, including pre-labour rupture of membranes, gestational diabetes, suspected big baby, low fluid at term, isolated hypertension at term, twins, being “due”, or being “overdue” (Mozurkewich, Chilimigras, Koepke, Keeton, & King, 2009; Cohain, n.d.; Mandruzzato et al., 2010).
“membrane sweeping is a procedure meant to induce labour so that the client won’t be induced later”
Membrane sweeping: Fred Flintstone manipulating your physiology
Membrane sweeping involves the provider inserting their gloved hand into a mother’s vagina and manually stretching open the cervix and then running their finger around the opening of the cervix to separate the amniotic sack from the lower uterine segment. Caregivers will say it feels much like separating Velcro.

This procedure has the potential to trigger labour because it releases extra prostaglandins at the cervix. If the membrane sweep results in a shorter cervix, then it doesn’t make any difference in whether the mother is subsequently induced, but it does decrease the incidence of c-section. However, membrane sweeping is much more likely to result in cervical lengthening – which is predictive of NOT going into labour (Tan, Khine, Sabdin, Vallikkannu, & Sulaiman, 2011).
Prostaglandins are one of many important hormones that are needed for labour and birth. As pregnancy progresses and it’s getting time for the baby to be born, there are complex processes that prepare and protect the baby and are necessary for labour to commence. For example, the cervix and the uterus develop prostaglandin receptors so that necessary prostaglandins have a place to “land” or “connect” so that they can do their job. The uterus develops an abundance of oxytocin receptors so that this love hormone that is produced in the brain can connect with the uterus and cause contractions. The baby’s brain develops oxytocin receptors, which is neuro-protective for the journey ahead. There is an increase in estrogen, which activates the uterus for delivery. There are inflammatory processes within the uterus that help to mature the baby’s lungs to prepare for breathing on the outside. The baby’s brain develops increased epinephrine receptors to protect it from any gaps in oxygen during the birth. The mother’s brain develops endorphin receptors for natural pain relief. And there is an increase in prolactin to prepare the mother for breastfeeding and bonding. (Buckley, 2015)
When considering the finely-tuned and delicate interplay of complex and specific processes that brings the baby earth-side, a manual stretch-and-sweep at term without any medical indication is like getting Fred Flintstone to program an app that regulates the autonomic nervous system. It’s a crude, blunt instrument inserted into a complex system with the intention of bypassing evolutionarily necessary adaptive processes to cut the pregnancy short by a possible few days.
Let’s try to induce labour so we don’t have to induce labour
A Cochrane Review (Bouvain, Stan, & Irion, 2005) evaluated available studies comparing membrane sweeping to no sweeping. In general, this procedure can reduce the duration of pregnancy by up to three days. However, the authors noted that only small studies showed this reduction in pregnancy duration whereas larger studies didn’t, suggesting some bias. Because membrane sweeping doesn’t usually lead to immediate labour, it is not recommended when the need to get the baby out is urgent. Its primary use is to “prevent” a longer gestation and therefore an induction by more risky means.
A stretch-and-sweep is a procedure that is meant to induce labour so that you won’t be induced later. The Society of Obstetricians and Gynaecologists of Canada wrote in their 2013 Practice Guideline, which was reaffirmed in 2015, that “routine sweeping (stripping) of membranes promotes the onset of labour and that this simple technique decreases induction rates.”
Again: membrane sweeping is a procedure meant to induce labour so that the client won’t be induced later.
It assumes that the later induction is non-negotiable and the client’s best hope is that this early induction “saves” her from the risks of the later induction.
This is no different than all those “natural” inductions that are employed when trying to induce labour so the mother doesn’t have experience an induction – or the challenge of just declining the planned induction. It takes the approach that planned inductions are non-negotiable. Of course, mothers may chose a natural induction as a means of expediting the births of their babies for a number of reasons and I fully support their autonomy and choice to do so.
If there is a medical need to get the baby out to preserve its or its mothers life, then this dyad should be under medical supervision and receiving the best medical care possible. We need to critically evaluate the mentality that says, “let’s try to induce so we don’t have to induce”.
We’ve bought into a culture where non-evidence-based time limits and spurious reasons are given for booking inductions that don’t line up with the science. Rather than supporting mothers in exploring the science, doing a targeted risk/benefit analysis based on her particular situation, and supporting the mother in informed decision making, we line up the early inductions hoping to out-smart, out-wit, and out-play the medical providers who routinely induce based on outdated information or habit or hospital protocols that are based in their insurance risk-management strategy.
If this procedure is not recommended when there is an urgent need to get the baby out (Bouvain et al., 2005) and its primary purpose is to prevent a later induction where the indication is a pregnancy continuing beyond the cut-off date of the caregiver or institution (SOGC, 2013), then it has no medical indication.
What else did the Cochrane Review find?
There was a high level of bias in many of the studies, in part, because there could be no blinding. The clinicians knew they were performing the procedure and the clients knew they’d received it due to discomfort and pain
It was an out-patient procedure meaning there was no urgent reason for the induction
It did not generally lead to labour within 24 hours
No difference in oxytocin augmentation, use of epidural, instrumental delivery, caesarean delivery, meconium staining, admission to the NICU, or Apgar score less than seven at five minutes between sweeping and non-sweeping. This means it didn’t show any benefit
No difference in pre-labour rupture of membranes, maternal infection or neonatal infection. However, it’s worth noting that the non-sweeping participants were subject to routine obstetrical services that includes many vaginal exams that increase pre-labour rupture of membranes and infection (Maharaj, 2007; Zanella et al., 2010; Lenihan, 1984; Critchfield et al., 2013)
Significant pain in the mother during the procedure
Vaginal bleeding after the procedure
Painful contractions for the next 24 hours not leading to labour
What we have here is a routine that hurts the mother and has no significant benefit – aside from maybe possibly putting her into labour before another planned induction.
As the Cochrane Review discovered, the likely outcome of a membrane sweep is painful non-progressing contractions. This is often mis-interpreted as “labour” and the client is sent to the hospital for an induction anyway because she’s been “in labour” for 24-48 hours without progress. This is the epitome of a hijacked birth that turns a normal physiological process into a pathological one leading to the cascade of interventions, sometimes all the way up to an unwanted and unplanned caesarean for “failure to progress”. To convert the natural process into a pathological one is part of the classic definition of obstetrical violence (D'Gregorio, 2010).
They call it ‘birth rape’
For those who experienced this without their prior knowledge or consent, their comments overwhelmingly spoke of rape. This was especially pronounced in those with a history of prior rape. Studies confirm that those with a history of rape experience the routines of industrial birth differently than those without a history of sexual assault. For survivors, procedures that are uneventful for others can inadvertently put them “back in the rape” (Halvorsen, Nerum, Øian, & Sørlie, 2013).
Frankly, it’s unconscionable that any care provider would brazenly take the opportunity to manually manipulate a woman’s cervix, knowing it introduces risks and has the potential to hurt her, without the express knowledge and consent of the client following an informed choice discussion.
While membrane sweeping is intended to induce labour, it’s also used on labouring women to hurry things along. During labour, the cervix is being moved and thinned by the action of uterine muscles contracting and pulling the cervix up and around the baby’s head. The cervix is working hard and it’s tender. Many women will report that they screamed, cried ‘no’, tried to kick the provider’s hand away, or tried to crawl up the bed to get away from the invasive exam.
I remember one dark cold February night, years ago, when I was called to be with a family in labour. There was an ice storm and my trip there was dangerous and precarious. Eventually, my car slid into their street and managed to stop somewhere close to the driveway. I quietly entered the house to hear a mother in the throes of glorious, deep, active labour. I knew it wouldn’t be long before the baby arrived. I announced myself and tiptoed upstairs to see her on hands and knees with more blood than I would have expected on the towel beneath her. She said she invited her midwife to the birth and expected her to be there any minute. Soon enough, a beautiful baby boy gently emerged and landed safely into his daddy’s waiting hands. By the time the midwives arrived, the new family was tucked into bed enjoying a post-birth snack and cup of tea.
As the new family was bonding, I joined the midwives downstairs who were making notes in their client’s medical charts to make them some tea and offer a snack. I overheard one midwife say, “Oh yeah, when I was here earlier, she was about 6cm so I did a stretch-and-sweep”.
“Oh yeah.
Now I remember.
She was in active labour so I did an invasive and painful procedure to speed things up during a dark and dangerous ice storm.
Without her knowing I would do that.”
This is nothing but reckless cruelty. Yet this kind of cruelty permeates maternity services where women are routinely hurt for the sole purpose of interfering in their physiology and the safety of the birth process in order to get the baby out before they do even more risky and dangerous things.
And that is why I would like to see the ROUTINE, WITHOUT MEDICAL INDICATION membrane sweep removed from obstetrical and midwifery practice. It shouldn’t be the luck of the draw that a pregnant client gets one of the “good ones” who only induces a client when there is a medical need, with an informed choice discussion, and full consent.
To return to my original question: what is it about membrane sweeping that is so cherished that challenging it generates death threats?
It’s a deeply embedded ritual in a toxic medical culture that presumes to take authority over a pregnant woman’s sexual organs for the purpose of dominating the physiological process and then becoming a hero to the interrupted physiology and complications that ensue. It’s about power and control. And challenging this is a dangerous act of sedition. Those who do this to their clients like being the hero and clients who defend this need to believe they were saved from something – otherwise the truth is just too awful.
Make wise choices.
Much love,
Mother Billie
#endobstetricalnonsense #informedconsent #obstetricalviolence #membranesweeping #stretchandsweep #withoutconsent #birthrape #failuretoprogress
References
Better Outcomes Registry Network. (BORN). 2013. Provincial Overview of Perinatal Health in 2011–2012.
Boulvain, M., Stan, C. M., & Irion, O. (2005). Membrane sweeping for induction of labour. Cochrane Database of Systematic Reviews, (1).
Buckley, S. J. (2015). Hormonal physiology of childbearing: Evidence and implications for women, babies, and maternity care. Washington, DC: Childbirth Connection Programs, National Partnership for Women & Families.
Cohain, J. S. Reducing Inductions: Lack of Justification to Induce for “Postdates”.
Critchfield, A. S., Yao, G., Jaishankar, A., Friedlander, R. S., Lieleg, O., Doyle, P. S., ... & Ribbeck, K. (2013). Cervical mucus properties stratify risk for preterm birth. PloS one, 8(8), e69528.
D'Gregorio, R. P. (2010). Obstetric violence: a new legal term introduced in Venezuela.
Halvorsen, L., Nerum, H., Øian, P., & Sørlie, T. (2013). Giving birth with rape in one's past: a qualitative study. Birth, 40(3), 182-191.
King, V., Pilliod, R., & Little, A. (2010). Rapid review: Elective induction of labor. Portland: Center for Evidence-based Policy.
Lenihan, J. J. (1984). Relationship of antepartum pelvic examinations to premature rupture of the membranes. Obstetrics and gynecology, 63(1), 33-37.
Leppert, P. C. (1995). Anatomy and physiology of cervical ripening. Clinical obstetrics and gynecology, 38(2), 267-279.
Maharaj, D. (2007). Puerperal pyrexia: a review. Part II. Obstetrical & gynecological survey, 62(6), 400-406.
Mandruzzato, G., Alfirevic, Z., Chervenak, F., Gruenebaum, A., Heimstad, R., Heinonen, S., ... & Thilaganathan, B. (2010). Guidelines for the management of postterm pregnancy. Journal of perinatal medicine, 38(2), 111-119.
Mozurkewich, E., Chilimigras, J., Koepke, E., Keeton, K., & King, V. J. (2009). Indications for induction of labour: a best‐evidence review. BJOG: An International Journal of Obstetrics & Gynaecology, 116(5), 626-636.
Osterman, M. J., & Martin, J. A. (2014). Recent declines in induction of labor by gestational age.
Rao, A., Celik, E., Poggi, S., Poon, L., & Nicolaides, K. H. (2008). Cervical length and maternal factors in expectantly managed prolonged pregnancy: prediction of onset of labor and mode of delivery. Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 32(5), 646-65.
Rayburn, W. F., & Zhang, J. (2002). Rising rates of labor induction: present concerns and future strategies. Obstetrics & gynecology, 100(1), 164-167.
Society of Obstetricians and Gynaecologists of Canada. SOGC. 2013. Clinical Practice Guideline, No. 296, Indution of Labour.
Tan, P. C., Khine, P. P., Sabdin, N. H., Vallikkannu, N., & Sulaiman, S. (2011). Effect of membrane sweeping on cervical length by transvaginal ultrasonography and impact of cervical shortening on cesarean delivery. Journal of Ultrasound in Medicine, 30(2), 227-233.
Zanella, P., Bogana, G., Ciullo, R., Zambon, A., Serena, A., & Albertin, M. A. (2010). Chorioamnionitis in the delivery room. Minerva pediatrica, 62(3 Suppl 1), 151-153.