
Why I don't do vaginal exams ~ Wisdom from a Traditional Birth Companion
I let my new client know what would happen when I arrived at her home when she was in labour. We talked about sanitation measures, spending time in the kitchen, setting up the pool, and where I could take a nap if she needed some privacy. I said I would not be doing any vaginal exams as I think they’re rude, and she wept with relief.
I specialise in trauma and the majority of my clients are refugees from the medical system, running from ritual abuse and routines that protect the industry. They want someone to mentor them through to a healthy birth without the traps and trappings of the industry that removed their choice, and violated their autonomy and their dignity.
As a traditional birth attendant, I don’t do vaginal exams.

I was talking with my new client about what would likely happen when I arrived at her home when she was in labour. We talked about sanitation measures, spending time in the kitchen, setting up the pool, and where I could take a nap if she needed some privacy. I said I would not be doing any vaginal exams as I think they’re rude, and she wept with relief.
I specialise in trauma and the majority of my clients are refugees from the medical system, running from ritual abuse and routines that protect the industry. They want someone to mentor them through to a healthy birth without the traps and trappings of the industry that removed their choice, and violated their autonomy and their dignity.
We won’t go into the history of obstetrics that began with the burning of witches (midwives and healers), the rise of the man-midwife, the development of lying-in hospitals, and eventually the wholesale co-opting and medicalisation of birth. Suffice it to say that obstetrics and hospitalisation didn’t “save” women and babies (1). It created untold harm and mortality until they learned better infection control and saner behaviours. Today, it’s still leaving a trail of destruction as about 1/3 of their clients are traumatised (2,3,4) and about 1 in 8 enter parenthood with postpartum post-traumatic stress disorder (5,6,7). Suicide is a leading cause of maternal death in the first year and is highly correlated to trauma (8,9,10,11,12,13,14,15,16). It’s an industry out of control with unjustifiable caesarean rates, dangerous inductions for spurious reasons, and wholesale overuse of medications and interventions.
What women didn’t notice in this process of medicalisation and co-opting of their physiology for profit is that the medical industry took ownership of their vaginas once they became pregnant. Pregnancy transfers ownership of the vagina from the woman to the industry. Midwifery and obstetrical regulations stipulate that inserting an instrument, hand, or finger beyond the labia majora is a restricted practice sanctioned by legislation (17). To test this, see how long it takes for someone in the industry to file a Cease and Desist or start a campaign of persecution for the purpose of prosecution if they catch wind of anyone but one of their own sticking their fingers up there. No one but an insider sticks their fingers into their territory. It doesn’t matter who the mother gives her permission and consent to - it must be a member of the priesthood of modern medicine.
Of course, in their benevolence, they’re generally quite accommodating where partners are concerned, because most partners are male and obstetrics is exceedingly misogynistic. They value the needs and the pleasures of the D.
As a traditional birth attendant, I don’t do vaginal exams. For one thing, it’s considered a restricted practice for just the medical pundits and not doing them with my clients keeps the industry players somewhat placated knowing I’m not intruding into their turf. But the real reason is because I think they’re completely unnecessary and wouldn’t do them even if the medical folks begged me to under the guise that it would make birth safer.
To better understand the offence of the routine vaginal exam, we have to go back in time to when the male-midwife moved into the sanctity of women-centred birth and the domain of the midwife. It was profitable. And they convinced the public that they would provide a superior service based on the cultural belief of the time that women were disadvantaged by an inferior intellect and a predilection for sorcery (18,19). They also brought with them the medical perspective that women were an error of nature and that the world, and thus its inhabitants, were but a machine that could be best understood by coming to know its parts in isolation of the whole.
And so began dissection, mechanisation, and reducing birthing women to their parts. She became a womb expelling a foetus through a vagina. Think of today’s obstetrical “power, passenger, passage” perspective on how birth unfolds. Not much has changed in 400 years.
By sticking their fingers up there, they discovered that the cervix opens to expel the foetus. Oh, happy day! From the morgue to the birth suite, physician fingers were poking everything. Throughout the early and mid 1800’s, the infection rate in some hospitals soared as high as 60% from the mysterious childbed fever, with death rates as high as 1 in 4 (20). Nothing the doctors did was contributing to this mystery as physicians were gentlemen and gentlemen didn’t carry germs (21). And once they did accept that their filthy practices were killing women, rather than abandon the idiocy of penetrating their patients in labour, they eventually figured out how to make it less dangerous.
The practice of obstetrics has always been highly resistant to change and common sense. After all, they’ve had 400 years to figure things out and women are still birthing on their backs!
Once it was discovered that the cervix dilates as part of the labouring process, the medical industry has been fixated on that bit of tissue and made it the focus of their entire assembly line drive-through everyone-gets-what’s-on-the-menu service. That bit of tissue determines how the ward allocates services, whether the client will be permitted to stay, and how long she’ll be allowed to use their services before the next client needs the bed.
Thanks to Dr. Emanuel Friedman, who examined the cervices of 500 sedated first-time mothers in the 1950’s and plotted their dilation on a graph and matched it to the time of their birth – we now have the infamous Friedman’s Curve and the partogram.

© Evidence Based Birth
The partogram is a graph that plots cervical dilation and descent of the foetal head against a time-line. When the graph indicates that progress is slower than is allowable according to the particular chart chosen by their institution, then the practitioner is called upon to administer various interventions to speed things up to keep the labour progressing well, aka, profitably. Should these acceleration measures fail to produce a baby in a timely manner or cause foetal distress, then a caesarean section is the solution. “Failure to progress”, and the accompanying foetal distress that is often a consequence of those acceleration measures, are the leading causes of a primary caesarean (22).

Obstetrical partogram
In addition to clearing the bed for the next client, obstetrics has another reason for expediting labour. The more vaginal exams a woman receives, the greater the likelihood she’ll develop a uterine infection (23). So, once they start the poking, they need to get the baby out before their prodding adds another problem for them to solve.
In the absence of a medical situation, routine vaginal exams in labour are for the purpose of charting in order to maintain a medicalised standard of modern technocratic birth.
A labouring client will not be admitted to a hospital without a vaginal exam to determine if her dilation is far enough along for their services (unless she’s clearly pushing). And this isn’t necessarily a bad thing. Early admission to the hospital results in more interventions and more caesareans than later admission (24). This is a business and time is money.
A regulated midwife attending a homebirth will likewise perform a vaginal exam upon arrival at the client’s home to determine if the client is far enough along to warrant their limited resources and time by staying and beginning the partogram or leaving and waiting to be called back later. They must also follow the rules of the hospital at which they have privileges or their regulatory agency and transport for augmentation/acceleration if the partogram shows a significant variation.
All of this is predicated on the outdated and obsolete notion that women are machines and birth is a linear process. The only thing a vaginal exam reveals is where the cervix is sitting at that particular moment and how it’s interpreted by that particular practitioner. Women are not machines and birth is not linear. Just like any mammal, birth can be slowed, stopped, or sabotaged by an unfavourable environment or reckless attendants. I’ve said for years that it’s so easy to sabotage a good birth, it’s embarrassing.
“Years ago, I was with a first-time mother planning a family-centred homebirth. She was on the clock and had a deadline. At 42 weeks gestation, she had until midnight that night to produce a baby in order to have a midwife-attended homebirth. After that, she was expected to report to the hospital for a chemical induction. As her contractions built throughout the day, her preferred midwife arrived and labour was progressing well. She was enjoying the process and the camaraderie of her sisters-in-birth. Eventually, one of the vaginal exams revealed a cervical dilation of 8 cm, indicating it was time to call in the 2nd midwife. Only, it was a midwife that had routinely upset the mother throughout pregnancy with requests for various tests and talk of all the dangers of declining routine testing. Upon learning this midwife was coming to the birth, labour slowed.
Soon enough, the 2nd midwife arrived and assumed authority over the birth process and insisted on repeated vaginal exams for the purpose of staying within the parameters of the partogram. Her vaginal exams were excruciating, no doubt because she was trying to administer a non-consenting membrane stripping as an intervention to address the slowed and almost non-existent contractions. Eventually, an exam revealed a dilation of only 6 cm. After several more hours of “torture” (according to this mother’s recount) to keep labour going rather than just leaving the mother to rest and accepting that this labour had been hijacked and needed time to regroup and restart, dilation regressed to 4 cm and the mother eventually ended up acquiescing to a hospital transfer, and experienced an all-the-bells-and-whistles birth, trauma, and postpartum PTSD.
This mother’s subsequent birth a couple of years later didn’t include inviting midwives and unfolded as it was meant to. After a day of productive and progressing labour that was clearly evident without sticking fingers up her vagina, she eventually got tired and labour slowed and stopped. She went to bed and I went home. When she woke up, labour resumed and a baby emerged swiftly and joyously. As it turns out, for her, she has a baby after a good sleep with people she trusts.”
What about the routine vaginal exams in late pregnancy? Glad you asked!
Since they don’t have good predictive value, meaning they won’t diagnose when labour will begin, how long it will take, or whether the woman’s pelvis will accommodate that particular baby prior to labour, they have 2 functions.
The first is to plan and initiate your induction.
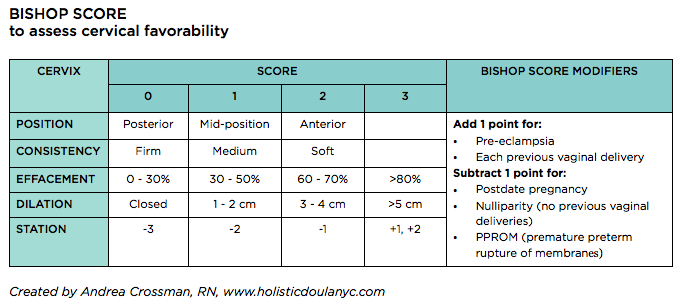
A cervical exam provides information that is measured against a Bishop Score. A Bishop Score provides a predictive assessment on whether an induction is likely to result in a vaginal birth or is more likely to result in a caesarean for “failure to progress”. A cervix that scores higher is more likely to respond to an induction whereas a lower score indicates a less favourable outcome (25). Further, a vaginal exam allows the practitioner to begin the induction process with a membrane stripping/stretch-and-sweep.
The second purpose for routine vaginal exams in pregnancy is to build in sexual submission. It reaffirms the power dynamic where someone who is not the woman’s intimate sexual partner is allowed to penetrate her genitals at will. It makes their job much simpler once she’s is in labour. She has been trained to accept this violation.
A vaginal exam during labour might rarely be indicated when there is a problem that requires more information. A vaginal exam can help determine if there’s a possible cord prolapse requiring immediate medical attention, or can asses the position and descent of the baby to help suggest strategies to encourage the baby to move into a better position. However, when a labour is spontaneous, meaning it hasn’t been induced by any mechanical, chemical, or “natural” means, the labour isn’t augmented with artificial rupture of membranes or synthetic oxytocin, and the labouring woman is untethered and free to move as her body indicates, complications are far less likely.
Throughout my 35 years in supporting birthing families, I can say that babies do indeed come safely and spontaneously out of vaginas when there’s no one sticking their fingers up there. And they tend to come more quickly. Routine vaginal exams don’t contribute to the safety of the mother/baby. However, they do add to the safety of the practitioner who is tasked with placating the technocratic gods who demand they follow protocols and keep the wheels of the business running on track.
My reasons for not doing vaginal exams, even if the the technocratic gods gave their blessing, include:
They’re rude
They’re unnecessary
They shift the locus of power from the birthing woman to the person with the gloves
They introduce the potential for infection
They interrupt labour and can sabotage a good birth
They often hurt
They can traumatise the cervix
They can traumatise the mother
They can impact the experience of the baby
There are so many simpler ways to determine how labour is progressing
I don’t practice medicine or midwifery or engage in its absurdities
I really am not that interested in other people’s vaginas
Let’s talk about when labour does veer from a normal physiological process.
When the power dynamic places the labouring and birthing mother in charge of the experience, it actually becomes a safer and simpler process. She is the one who is experiencing the labour and birth and is the one relaying information. Only she is in direct communication with her baby. She is the one who knows when labour has exceeded her resources and she needs medical help, pharmacologic pain relief, or the reassurance of the technocratic model.
Of course, not all births unfold simply. However, my experience over these many years is that when women are not expected to submit to exams for the purpose of charting and the subsequent limitations imposed by those charts, birth unfolds a lot more simply far more often.
Much love,
Mother Billie ❤️
Endnotes
Tew, Marjorie. Safer childbirth?: a critical history of maternity care. (2013). Springer.
Garthus-Niegel, S., von Soest, T., Vollrath, M. E., & Eberhard-Gran, M. (2013). The impact of subjective birth experiences on post-traumatic stress symptoms: a longitudinal study. Archives of women's mental health, 16(1), 1-10.
Creedy, D. K., Shochet, I. M., & Horsfall, J. (2000). Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth, 27(2), 104-111.
Schwab, W., Marth, C., & Bergant, A. M. (2012). Post-traumatic stress disorder post partum. Geburtshilfe und Frauenheilkunde, 72(01), 56-63.
Montmasson, H., Bertrand, P., Perrotin, F., & El-Hage, W. (2012). Predictors of postpartum post-traumatic stress disorder in primiparous mothers. Journal de gynecologie, obstetrique et biologie de la reproduction, 41(6), 553-560.
Beck, C. T., Gable, R. K., Sakala, C., & Declercq, E. R. (2011). Posttraumatic stress disorder in new mothers: Results from a two‐stage US National Survey. Birth, 38(3), 216-227.
Shaban, Z., Dolatian, M., Shams, J., Alavi-Majd, H., Mahmoodi, Z., & Sajjadi, H. (2013). Post-traumatic stress disorder (PTSD) following childbirth: prevalence and contributing factors. Iranian Red Crescent Medical Journal, 15(3), 177-182.
Oates, M. (2003). Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. British medical bulletin, 67(1), 219-229.
Oates, M. (2003). Suicide: the leading cause of maternal death. The British Journal of Psychiatry, 183(4), 279-281.
Cantwell, R., Clutton-Brock, T., Cooper, G., Dawson, A., Drife, J., Garrod, D., Harper, A., Hulbert, D., Lucas, S., McClure, J. and Millward-Sadler, H. (2011). Saving Mothers' Lives: Reviewing maternal deaths to make motherhood safer: 2006-2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG: an international journal of obstetrics and gynaecology, 118, 1-203.
Austin, M. P., Kildea, S., & Sullivan, E. (2007). Maternal mortality and psychiatric morbidity in the perinatal period: challenges and opportunities for prevention in the Australian setting. Medical Journal of Australia, 186(7), 364-367
Palladino, C. L., Singh, V., Campbell, J., Flynn, H., & Gold, K. (2011). Homicide and suicide during the perinatal period: findings from the National Violent Death Reporting System. Obstetrics and gynecology, 118(5), 1056.
Grigoriadis, S., Wilton, A.S., Kurdyak, P.A., Rhodes, A.E., VonderPorten, E.H., Levitt, A., Cheung, A. and Vigod, S.N. (2017). Perinatal suicide in Ontario, Canada: a 15-year population-based study. Cmaj, 189(34), E1085-E1092.
CEMD (Confidential Enquiries into Maternal Deaths) (2001) Why Mothers Die 1997–1999. London: Royal College of Obstetricians and Gynaecologists.
Sareen, J., Cox, B. J., Stein, M. B., Afifi, T. O., Fleet, C., & Asmundson, G. J. (2007). Physical and mental comorbidity, disability, and suicidal behavior associated with posttraumatic stress disorder in a large community sample. Psychosomatic medicine, 69(3), 242-248.
Hudenko, William, Homaifar, Beeta, and Wortzel, Hal. (July 2016). The Relationship Between PTSD and Suicide. PTSD: National Center for PTSD, U.S. Department of Veterans Affair.
Act, Ontario Midwifery. "SO 1991, c. 31." (1991).
Smith Adams, K. L. (1988). From 'the help of grave and modest women' to 'the care of men of sense': the transition from female midwifery to male obstetrics in early modern England. (Master’s thesis, Portland State University.
Burrows, E. G., & Wallace, M. (1998). Gotham: a history of New York City to 1898. Oxford University Press.
Semmelweis, I. (1983). Etiology, concept, and prophylaxis of childbed fever. Carter KC, ed. Madison, WI.
Halberg, F., Smith, H. N., Cornélissen, G., Delmore, P., Schwartzkopff, O., & International BIOCOS Group. (2000). Hurdles to asepsis, universal literacy and chronobiology-all to be overcome. Neuroendocrinology Letters, 21(2), 145-160.
Caughey, A. B., Cahill, A. G., Guise, J. M., Rouse, D. J., & American College of Obstetricians and Gynecologists. (2014). Safe prevention of the primary cesarean delivery. American journal of obstetrics and gynecology, 210(3), 179-193.
Curtin, W. M., Katzman, P. J., Florescue, H., Metlay, L. A., & Ural, S. H. (2015). Intrapartum fever, epidural analgesia and histologic chorioamnionitis. Journal of Perinatology, 35(6), 396-400.
Kauffman, E., Souter, V. L., Katon, J. G., & Sitcov, K. (2016). Cervical dilation on admission in term spontaneous labor and maternal and newborn outcomes. Obstetrics & Gynecology, 127(3), 481-488.
Vrouenraets, F. P., Roumen, F. J., Dehing, C. J., Van den Akker, E. S., Aarts, M. J., & Scheve, E. J. (2005). Bishop score and risk of cesarean delivery after induction of labor in nulliparous women. Obstetrics & Gynecology, 105(4), 690-697.
The system isn’t broken - but its people are
One third of birthing parents has a traumatic birth.
“The system is broken.”
One in 8 new parents enters parenthood with postpartum PTSD from the experience.
“The system is broken.”
Depending on where you live, one third, one half, or almost everyone has a surgical birth.
“The system is broken.”
One in 6 women are abused during their births.
“The system is broken.”
If we say it enough, we might believe it. However, the “system” is decidedly NOT broken. It is doing exactly what it was set up to do by any means available to it.
One third of birthing parents has a traumatic birth.[i] [ii] [iii]
“The system is broken.”
One in 8 new parents enters parenthood with postpartum PTSD from the experience.[iv]
“The system is broken.”
Depending on where you live, one third, one half, or almost everyone has a surgical birth.[v]
“The system is broken.”
One in 6 women are abused during their births.[vi]
“The system is broken.”

If we say it enough, we might believe it. However, the “system” is decidedly NOT broken. It is doing exactly what it was set up to do by any means available to it.
The “system” is how we deliver maternity services. It began when male-midwives, those physicians who broke social etiquette, began attending women in birth. They were barbaric in means because they were sanctioned by the Catholic church to carry sharp instruments that women were forbidden to use. Male barber-surgeons, the Chamberlains, invented the forceps but kept their secret hidden for a century. A few centuries of witch hunts where midwives and female healers were persecuted and executed taught the public to shy away from learning these skills – if they were women. The collusion of religion and medicine ensured that men gained and maintained a monopoly over sick care and what women were allowed to do with their own bodies.[vii]
Eventually, through clever marketing, the male midwife became the preferred attendant as they were considered superior in intellect.[viii] [ix] Women were forbidden to attend universities, practice medicine, or serve in leadership in religions that ruled the western politic, thus unable to influence how women were treated in childbirth.[x]
Sure enough, these clever men discovered how much more profitable it was to bring birthing clients to them rather than going out to their homes.[xi] And so emerged the ‘lying-in’ hospital. The wholesale slaughter of women in these death traps was on par with the witch hunts of a few centuries prior. One in ten women died from puerperal fever, brought on by the unwashed hands of physicians who went from cadaver to the birthing vagina.[xii] Despite the protests of the offensive Semmelweis to wash their hands, ego and elitism prevented them from adopting this simple strategy for many more years thus ensuring the needless deaths of countless more women.[xiii]

Ignaz Semmelweis washing hands with chlorine-water, 1846
Once chloroform and other means of anesthesia were available for use in childbirth, the medical societies lobbied the government to grant them exclusive access. Not that they were any more qualified to use these powerful drugs than any other discipline, they merely had the ear of those in power who made these decisions.[xiv] Next followed the most effective smear campaign in all of history to drive midwives and alternative healing modalities out of business. [xv] [xvi] By the end of WW2 the campaign was almost complete. Next came effective lobbying to ensure governments were only favourable to their approach and the money, legislations, and endorsements flowed to hospital based technocratic birth where the obstetrician is royalty.
Even today, midwives around the world are persecuted and legislated out of business for offering client-centred care and serving women outside of hospitals.

Leaning heavily on Henry Ford’s conveyor belt system of turning out cars, optimisations and standardisations were implemented to cut costs, increase revenue, and turn the business of birth into a well-oiled machine.[xvii]
What we have is an effective system of profit for those industry players who set it up this way.
Of course, women are abused in birth! It’s an effective means of getting them to submit to a routine, one-size-fits-all, conveyor belt, in-and-out, profitable baby factory.
Even the current schedule of prenatal visits has no basis in science, evidence, or benefit. It was created by those same male-midwives who took a good thing and made it $tandard. Certainly, diagnosing and treating medical issues is an important healthcare strategy, whether pregnant or not. In light of the evidence that today’s current schedule and routines have not produced the promised results of healthier pregnancies or births, the industry recommended and implemented a strategy to convince the public that the process of pregnancy could not be trusted to stay normal without their surveillance.[xviii]
Now let’s talk about the people.
Some people enter this industry because it’s proven itself as a profitable endeavour. Obstetrics includes a great deal of power and control over a physiological process that in most cases would unfold quite simply without them. This appeals to some people. It’s a position of elitism and sits higher on the social hierarchy. There’s nothing to see there. Nothing to reach. Nothing to change.
And some enter this industry because they believe they have something valuable to offer during one of the most sacred and vulnerable times in a person’s life. They believe in the importance of how new humans are greeted into this world.
But because they have entered a highly successful system, they witness and sometimes participate in horrific abuses of mothers and babies. Some are broken by this and are the walking and working wounded, grappling with trauma, burnout, PTSD, and even suicidal ideation. Some survive and continue doing the best they can without the learned skillset of trauma-informed care that protects them and their clients. And some become part of the system of abuse and profit as their initial purpose is co-opted by internalised patriarchy and misogyny.
But what’s to be done with those who are broken and those who are merely surviving? The system doesn’t care if they burnout and leave. Players are easily replaced by new inductees at beginner salaries. It was never set up to take care of anyone. It was set up as a profitable means of co-opting physiology for profit based on fear and coercion.
“What we have is a medical system that is literally killing people through suicide.”
Break time. Nature and birth are not always kind. Women have always benefited from the companionship and knowledge of their midwives. And when events became problematic, skilled surgeons and expert paediatricians have brought hope and life where there was once only death. This post only speaks to the system of facility-based birth that currently exists within a patriarchal, misogynistic, and technocratic paradigm.

Back to the people.
‘Burnout’ consists of three features
Emotional exhaustion – feeling emotionally depleted from being overworked
Depersonalisation and cynicism – unfeeling towards patients and peers with often negative, callous, and detached responses
Reduced personal efficacy – a reduced sense of competence or achievement in one’s work
Burnout, compassion fatigue, and trauma are often intermingled in the academic literature so it’s hard to get a sense of the enormity of the issue. However, we do know this:
Physicians
Female physicians have higher rates of burnout and less work satisfaction than males[xxiii]
Physicians have the highest rate of suicide of any profession[xxiv]
General population - 12.3 per 100,000
Physicians -28 to 40 per 100,000
Equal numbers of male and female physicians complete a suicide
Midwives
Midwives around the world report rates of burnout from 20%[xxv] to 65%[xxvi]
One third of midwives have clinical PTSD[xxvii]
Witnessing abusive care of patients creates more severe PTSD[xxviii]
Nurses
35% of labour and delivery nurses have moderate to severe secondary traumatic stress[xxix]
Witnessing or participating in abusive births is a direct contributor to trauma
24% higher rate of suicide than those outside the profession[xxx]
Nurses and Midwives
Female 192% more likely to complete suicide than females in other occupations
8.2 per 100,000 vs 2.8 per 100.000
Male 52% more likely to complete suicide than males in other occupations
22.7 per 100,000 vs 14.9 per 100.000
Male 196% more likely to complete suicide than female colleagues
22.7 per 100,000 vs 8.2 per 100.000[xxxi]
Doulas
Half of doulas report burnout[xxxii] where traumatic incidences and witnessing the mistreatment of labouring clients were direct causes of burnout. Secondary trauma causes doulas to leave the profession early, especially in light of institutional hostility, low income, and routine abuses of their clients[xxxiii]
From the client’s perspective, the simple answer is to birth outside the system.[xxxiv] It’s a reasonable option – unless you’ve drunk the Kool Aid and feel these parents are a danger to their foetus and must be punished through disrespectful care[xxxv] and calls to Childrens Apprehension Services. If enough clients choose an alternative to the system, then simple economics will drive change to bring back the customers.
Birthing families are paying a steep price for system-driven birth. High rates of trauma, postpartum PTSD, postpartum depression and anxiety, relationship breakdowns, and postpartum suicide.[xxxvi] [xxxvii] [xxxviii] [xxxix] [xl] [xli] What we have is a medical system that is literally killing people through suicide.
So, what to do with the crippling loss of health and wellness in those professionals who chose to enter the system to support families in a humane and compassionate manner? Is it even possible to bring back those who have lost their way?
Because the system of institutionalised maternity services is predicated on a patriarchal and misogynistic paradigm of control and elitism, it will never take care of those who are on the front lines. We must learn to take care of ourselves and each other.
Many good and decent people entered into the system of technocratic birth services with all the requisite technical skills and a desire to make a difference in the lives of birthing families. What was missing from their education and skills development were those specific skills that would equip them to work in that environment without losing their soul, their identity, or their life.
Fortunately, the same research that identifies the many problems with this delivery system of services, also identifies the many solutions. For those that are on a journey out of trauma and professional burnout towards recovery and professional efficacy, there are proven strategies that can help walk you towards recovery and wholeness. You can learn
A research-based understanding of the causes and consequences of birth trauma in the birthing client and how to avoid participating
A thorough understanding of secondary and vicarious trauma and its effects in healthcare providers
How to build neurological, biological, psychological, social, cultural, and structural resilience
The positive impact of affective empathy and how to use it
How to employ a trauma-informed approach with clients and peers that improves clinical accuracy, client and professional well-being, and reduces burnout, medical mistakes, and litigation
A knowledge of therapeutic modalities that are specific to trauma
Recovery is possible for those who seek it. While the system runs perfectly as it was designed to, it’s also possible that with enough recovered, equipped, and healthy participants we might see some significant changes that actually helps it to live up to its marketing of “healthy baby healthy mother”. In time, it might even include “healthy professionals”.
I’ve got the science. I’ve got the experience. And I’ve got the tools to help. Let’s do this together.
Much love,
Mother Billie
Endnotes
[i] Garthus-Niegel, S., von Soest, T., Vollrath, M. E., & Eberhard-Gran, M. (2013). The impact of subjective birth experiences on post-traumatic stress symptoms: a longitudinal study. Archives of women's mental health, 16(1), 1-10.
[ii] Creedy, D. K., Shochet, I. M., & Horsfall, J. (2000). Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth, 27(2), 104-111.
[iii] Schwab, W., Marth, C., & Bergant, A. M. (2012). Post-traumatic stress disorder post partum. Geburtshilfe und Frauenheilkunde, 72(01), 56-63.
[iv] Montmasson, H., Bertrand, P., Perrotin, F., & El-Hage, W. (2012). Predictors of postpartum post-traumatic stress disorder in primiparous mothers. Journal de gynecologie, obstetrique et biologie de la reproduction, 41(6), 553-560.
[v] Boerma, T., Ronsmans, C., Melesse, D. Y., Barros, A. J., Barros, F. C., Juan, L., ... & Neto, D. D. L. R. (2018). Global epidemiology of use of and disparities in caesarean sections. The Lancet, 392(10155), 1341-1348.
[vi] Vedam, S., Stoll, K., Taiwo, T. K., Rubashkin, N., Cheyney, M., Strauss, N., ... & Schummers, L. (2019). The Giving Voice to Mothers study: inequity and mistreatment during pregnancy and childbirth in the United States. Reproductive health, 16(1), 77.
[vii] Ehrenreich, B., & English, D. (2010). Witches, midwives, & nurses: A history of women healers. The Feminist Press at CUNY.
[viii] Smith Adams, K. L. (1988). From 'the help of grave and modest women' to 'the care of men of sense': the transition from female midwifery to male obstetrics in early modern England. (Master’s thesis, Portland State University.
[ix] Burrows, E. G., & Wallace, M. (1998). Gotham: a history of New York City to 1898. Oxford University Press.
[x] Minkowski, W. L. (1992). Women healers of the middle ages: selected aspects of their history. American journal of public health, 82(2), 288-295.
[xi] Tew, M. (2013). Safer childbirth?: a critical history of maternity care. Springer.
[xii] Loudon, I. (2000). The tragedy of childbed fever. New York, Oxford University Press.
[xiii] Tew, M. 2013, op. cit.
[xiv] Bonner, T. N. (1989). Abraham Flexner as critic of British and Continental medical education. Medical history, 33(4), 472-479.
[xv] Getzendanner, S. (1988). Permanent injunction order against AMA. JAMA, 259(1), 81-82.
[xvi] Weeks, John. (n.d.). “AMA ‘Thwarts’ Other Professions Practice Expansion and a Challenge to CAM-IM Fields”. The Integrator Blog. http://theintegratorblog.com/?option=com_content&task=view&id=73&Itemid=1
[xvii] Perkins, B. B. (2004). The medical delivery business: Health reform, childbirth, and the economic order. Rutgers University Press.
[xviii] Ball, J. (1993). The Winterton report: difficulties of implementation. British Journal of Midwifery, 1(4), 183-185.
[xix] Peckham, C. (2016). Medscape lifestyle report 2016: bias and burnout. New York, NY: Medscape.
[xx] Avery, Granger, M.D., (2017). The role of the CMA in physician health and wellness. Canadian Medical Association.
[xxi] Imo, U. O. (2017). Burnout and psychiatric morbidity among doctors in the UK: a systematic literature review of prevalence and associated factors. BJPsych bulletin, 41(4), 197-204.
[xxii] Wu, F., Ireland, M., Hafekost, K., & Lawrence, D. (2013). National mental health survey of doctors and medical students.
[xxiii] Peckham, C., 2016, op. cit.
[xxiv] T’Sarumi, O., Ashraf, A., & Tanwar, D. (2018). Physician suicide: a silent epidemic. Reunión Anual de la American Psychiatric Association (APA). Nueva York, Estados Unidos, 1-227.
[xxv] Henriksen, L., & Lukasse, M. (2016). Burnout among Norwegian midwives and the contribution of personal and work-related factors: a cross-sectional study. Sexual & Reproductive Healthcare, 9, 42-47.
[xxvi] Creedy, D. K., Sidebotham, M., Gamble, J., Pallant, J., & Fenwick, J. (2017). Prevalence of burnout, depression, anxiety and stress in Australian midwives: a cross-sectional survey. BMC pregnancy and childbirth, 17(1), 13.
[xxvii] Sheen, K., Spiby, H., & Slade, P. (2015). Exposure to traumatic perinatal experiences and posttraumatic stress symptoms in midwives: prevalence and association with burnout. International journal of nursing studies, 52(2), 578-587.
[xxviii] Leinweber, J., Creedy, D. K., Rowe, H., & Gamble, J. (2017). Responses to birth trauma and prevalence of posttraumatic stress among Australian midwives. Women and birth, 30(1), 40-45.
[xxix] Beck, C. T., & Gable, R. K. (2012). A mixed methods study of secondary traumatic stress in labor and delivery nurses. Journal of Obstetric, Gynecologic & Neonatal Nursing, 41(6), 747-760.
[xxx] Office for National Statistics. (2017). Suicide by occupation, England: 2011 to 2015.
[xxxi] Milner, A.J., Maheen, H., Bismark, M.M., & Spittal, M.J. (2016) Suicide by health professionals: a retrospective mortality study in Australia, 2001–2012. Medical Journal of Australia 205 (6): 260-265.
[xxxii] Naiman-Sessions, M., Henley, M. M., & Roth, L. M. (2017). Bearing the burden of care: emotional burnout among maternity support workers. In Health and Health Care Concerns Among Women and Racial and Ethnic Minorities (pp. 99-125). Emerald Publishing Limited.
[xxxiii] Roth, L. M., Heidbreder, N., Henley, M. M., Marek, M., Naiman-Sessions, M., Torres, J. M., & Morton, C. H. (2014). Maternity support survey: A report on the cross-national survey of doulas, childbirth educators and labor and delivery nurses in the United States and Canada.
[xxxiv] Holten, L., & de Miranda, E. (2016). Women׳ s motivations for having unassisted childbirth or high-risk homebirth: An exploration of the literature on ‘birthing outside the system’. Midwifery, 38, 55-62.
[xxxv] Vedam, S., Stoll, K., Rubashkin, N., Martin, K., Miller-Vedam, Z., Hayes-Klein, H., & Jolicoeur, G. (2017). The Mothers on Respect (MOR) index: measuring quality, safety, and human rights in childbirth. SSM-Population Health, 3, 201-210.
[xxxvi] Oates, M. (2003). Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. British medical bulletin, 67(1), 219-229.
[xxxvii] Oates, M. (2003). Suicide: the leading cause of maternal death. The British Journal of Psychiatry, 183(4), 279-281.
[xxxviii] Lewis, G. (2007). Saving mothers' lives: reviewing maternal deaths to make motherhood safer 2003-2005: the seventh report of the confidential enquiries into maternal deaths in the United Kingdom. CEMACH.
[xxxix] Austin, M. P., Kildea, S., & Sullivan, E. (2007). Maternal mortality and psychiatric morbidity in the perinatal period: challenges and opportunities for prevention in the Australian setting. Medical Journal of Australia, 186(7), 364-367.
[xl] Palladino, C. L., Singh, V., Campbell, J., Flynn, H., & Gold, K. (2011). Homicide and suicide during the perinatal period: findings from the National Violent Death Reporting System. Obstetrics and gynecology, 118(5), 1056.
[xli] Grigoriadis, S., Wilton, A. S., Kurdyak, P. A., Rhodes, A. E., VonderPorten, E. H., Levitt, A., ... & Vigod, S. N. (2017). Perinatal suicide in Ontario, Canada: a 15-year population-based study. Cmaj, 189(34), E1085-E1092.

Birth Hijacked – The Ritual Membrane Sweep
I’ve written about many topics over the years but nothing has ever generated as much discussion, opposition, and vitriol as challenging the cherished routine membrane sweep/stripping, aka stretch-and-sweep. A few years ago, I wrote a post about how I’d like to see the routine, prior-to-40-weeks, without-medical-indication membrane sweep banned from obstetrical and midwifery practice. I talked about its risks and the fact that the clients I worked with called it a sexual assault when done without consent
The post went viral and I received hate messages and emails from around the world defending this procedure. In general, the sentiment was that I should most definitely be having sexual relations with myself, after which, I should be locked up and forever silenced. I also heard from hundreds of women whose births were ruined by days of painful, non-progressing contractions triggered by a membrane sweep that ended up in a fully medicalised all-the-interventions arrival for their baby that they didn’t want. And horrifically, even more hundreds wrote to share their stories of non-consenting, painful, and violating membrane sweeping when there was no reason for it, aside from the care provider’s decision that they had agency over their patient’s vagina and could do what they wanted when they wanted.
So what is it about membrane sweeping that is so cherished that challenging it generates death threats?
Buckle up. Here we go again!

©Hanna-Barbera
I’ve written about many topics over the years but nothing has ever generated as much discussion, opposition, and vitriol as challenging the cherished routine membrane sweep/stripping, aka stretch-and-sweep.
A few years ago, I wrote a post about how I’d like to see the routine, prior-to-40-weeks, without-medical-indication membrane sweep banned from obstetrical and midwifery practice. I talked about its risks and the fact that the clients I worked with called it a sexual assault when done without consent
The post went viral and I received hate messages and emails from around the world defending this procedure. In general, the sentiment was that I should most definitely be having sexual relations with myself, after which, I should be locked up and forever silenced. I also heard from hundreds of women whose births were ruined by days of painful, non-progressing contractions triggered by a membrane sweep that ended up in a fully medicalised all-the-interventions arrival for their baby that they didn’t want. And horrifically, even more hundreds wrote to share their stories of non-consenting, painful, and violating membrane sweeping when there was no reason for it, aside from the care provider’s decision that they had agency over their patient’s vagina and could do what they wanted when they wanted.
That particular post was prompted by a brief encounter with a new mother. Her baby was little and we got talking. She told me how she went to her usual prenatal visit at 36 weeks and the doctor said it was time for a vaginal check to see how things were coming along. She thought that was an ok idea and stripped accordingly, lay down on the examining table and put her feet in the stirrups. However, rather than a simple vaginal exam, she experienced excruciating pain that had her crawling up the table trying to escape that probing hand. The doctor removed her bloodied glove and when this woman asked why she was bleeding, the doctor responded, “That should get things going”. This mother had experienced a non-consenting, unplanned, and unknowing stretch-and-sweep to start labour before she or the baby were ready. She went home bleeding and cramping and within a few days went into labour and birthed a baby that was not ready to breathe. The baby spent 3 days in the NICU and she was devastated. Her birth was hijacked by a damnable routine from someone who should have known better or at least given a damn.
Yes, that was obstetrical violence. However, the routine of membrane sweeping for the mere reason that the client is at term is a deeply embedded ritual in obstetrics and mimicked by some midwives. I don’t think there is one other procedure that so callously turns a normally progressing pregnancy into a pathological event than this heinous routine.
So what is it about membrane sweeping that is so cherished that challenging it generates death threats?
Routines are habits that help organise our days
Let’s begin with some clarity on what I’m challenging.
First and foremost, I am not challenging the right for a pregnant person to choose a membrane sweep as a means of expediting labour. I fully support an individual’s right and autonomy to choose what is best for them.
Secondly, I am not challenging this as a tool for expediting labour when there is a medical indication.
I am challenging the ROUTINE of membrane sweeping that is done by some care providers as part of their normal and usual prenatal “package”, without any hint that there is a reason to expedite the birth of the baby due to an emerging medical condition.
At your cervix, ma’am

Let’s take a tour of the cervix. The cervix is a narrow passage that sits at the lower end of the uterus extending into the vagina. The cervix changes throughout the menstrual cycle and serves an important function in fertility. During ovulation, the cervix produces sperm-friendly mucus and becomes softer and more open to facilitate sperm reaching the ovum. When not ovulating, it produces sperm-unfriendly mucus and makes it more difficult for sperm to pass through to the uterus.
In pregnancy, the cervix fills with mucus, which creates a barrier to help prevent infection from passing through to the uterus. The cervix remains closed and rigid (like the tip of your nose) and is about 3-5 cm. long.
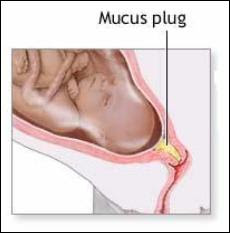
At term, in preparation for birth, the cervix will soften (like the inside of your cheek) due to the action of various hormones. The cervix is comprised of about 5-10% smooth muscle cells, which ensures it will stay closed and rigid throughout pregnancy. In preparation for labour, these muscle cells experience a programmed cellular death, which allows for the cervix to open (Leppert, 1995). The cervix will develop more oxytocin and prostaglandin receptors to help with the dilation process (Buckley, 2015). Prostaglandins, which are found abundantly in semen, ripens the cervix, digests the mucus plug, and promotes softening and shortening of the cervix.
Medical providers tend to give a great deal of attention to the cervix both prior to labour and in labour. It can provide some information that the medical folks find useful.
At term (around 40 weeks), the cervix can be felt to determine if it is ripening. Ripening means that the cervix is becoming softer, shorter, and is moving its position slightly forward. If so, it means that normal end-of-pregnancy hormones are doing their job. If not, it means that normal end-of-pregnancy hormones are doing their job, but they just haven’t gotten around to softening and shortening the cervix at the moment that a gloved hand is probing it.
This information is useful for planning an induction. A cervix that is shorter than 1.5 cm. is more predictive of spontaneous labour within the next 7-10 days than a longer cervix (Rao, Celik, Poggi, Poon, & Nicolaides, 2008). And a cervix that scores higher on the Bishop score is more predictive of an induction resulting in a vaginal birth rather than surgery (usually called “failure to progress”) (King, Pilliod, & Little, 2010). So that end-of pregnancy vaginal exam is about gathering information to plan your induction.
The other possibility for these routine (without medical indication) vaginal examinations in a healthy pregnancy is to develop submission and compliance in the client as she subjugates herself to the clinician by having her genitals penetrated by someone who is not her intimate partner.
Not too long ago, I was working with a postpartum client who was recovering from her birth experience. As a survivor of sexual assault she did not want anyone penetrating her genitals when she was labouring and giving birth and repeatedly told her midwife this. However, her midwife felt it was best for her to submit to vaginal exams in pregnancy to “get used to” them before she was in labour. Apparently, it never occurred to either of them that vaginal exams are optional and largely unnecessary for birthing a baby. In this case, the prenatal vaginal exams were for the purpose of building in submission and compliance so that the care providers could exercise agency over her body in labour.
Inductions: getting the baby out before it’s ready
An induction starts labour artificially before optimal hormonal physiology has prepared the baby and the mother for spontaneous birth. About 1 in 4 births begin by induction (BORN, 2013; Osterman & Martin, 2014). Although, there has been a slight decrease in inductions in recent years as fewer early-term inductions, meaning prior to 39 weeks, are performed. This has allowed more mothers to go into spontaneous labour without any additional adverse outcomes (Osterman & Martin, 2014). The cervix is one small part of the whole physiological process and since it can be reached easily by probing hands, it can provide a bit of information on whether an induction is likely to lead to a vaginal birth or is more likely to result in caesarean surgery.
There are lots of ways to artificially start labour before the mother or baby are ready. There are the so-called “natural” inductions:
Acupuncture and acupressure
Herbs and Homeopathy
Castor oil
Massage
Nipple stimulation
There are chemical inductions, which the literature calls “formal” inductions, as they require medical supervision:
Cervical ripening with prostaglandins
Intravenous synthetic oxytocin
And we have mechanical inductions, which also generally require medical supervision:
Artificial rupture of membranes aka “breaking the water”
Cervical ripening with a balloon catheter
Manual membrane sweeping/stripping, “stretch and sweep”
Ideally, an induction should only be suggested when the risks of staying pregnant outweigh the long and short-term risks of an induction. Depending on the method of induction those risks can include preterm birth, breathing problems in the baby, infection in the mother or baby, uterine hyper-stimulation, uterine rupture, fetal distress, breastfeeding failure, and rarely, death of either the mother or the baby.
Unfortunately, most inductions are done where the research affirms that the risks of an induction outweigh the risks of staying pregnant, including pre-labour rupture of membranes, gestational diabetes, suspected big baby, low fluid at term, isolated hypertension at term, twins, being “due”, or being “overdue” (Mozurkewich, Chilimigras, Koepke, Keeton, & King, 2009; Cohain, n.d.; Mandruzzato et al., 2010).
“membrane sweeping is a procedure meant to induce labour so that the client won’t be induced later”
Membrane sweeping: Fred Flintstone manipulating your physiology
Membrane sweeping involves the provider inserting their gloved hand into a mother’s vagina and manually stretching open the cervix and then running their finger around the opening of the cervix to separate the amniotic sack from the lower uterine segment. Caregivers will say it feels much like separating Velcro.

This procedure has the potential to trigger labour because it releases extra prostaglandins at the cervix. If the membrane sweep results in a shorter cervix, then it doesn’t make any difference in whether the mother is subsequently induced, but it does decrease the incidence of c-section. However, membrane sweeping is much more likely to result in cervical lengthening – which is predictive of NOT going into labour (Tan, Khine, Sabdin, Vallikkannu, & Sulaiman, 2011).
Prostaglandins are one of many important hormones that are needed for labour and birth. As pregnancy progresses and it’s getting time for the baby to be born, there are complex processes that prepare and protect the baby and are necessary for labour to commence. For example, the cervix and the uterus develop prostaglandin receptors so that necessary prostaglandins have a place to “land” or “connect” so that they can do their job. The uterus develops an abundance of oxytocin receptors so that this love hormone that is produced in the brain can connect with the uterus and cause contractions. The baby’s brain develops oxytocin receptors, which is neuro-protective for the journey ahead. There is an increase in estrogen, which activates the uterus for delivery. There are inflammatory processes within the uterus that help to mature the baby’s lungs to prepare for breathing on the outside. The baby’s brain develops increased epinephrine receptors to protect it from any gaps in oxygen during the birth. The mother’s brain develops endorphin receptors for natural pain relief. And there is an increase in prolactin to prepare the mother for breastfeeding and bonding. (Buckley, 2015)
When considering the finely-tuned and delicate interplay of complex and specific processes that brings the baby earth-side, a manual stretch-and-sweep at term without any medical indication is like getting Fred Flintstone to program an app that regulates the autonomic nervous system. It’s a crude, blunt instrument inserted into a complex system with the intention of bypassing evolutionarily necessary adaptive processes to cut the pregnancy short by a possible few days.
Let’s try to induce labour so we don’t have to induce labour
A Cochrane Review (Bouvain, Stan, & Irion, 2005) evaluated available studies comparing membrane sweeping to no sweeping. In general, this procedure can reduce the duration of pregnancy by up to three days. However, the authors noted that only small studies showed this reduction in pregnancy duration whereas larger studies didn’t, suggesting some bias. Because membrane sweeping doesn’t usually lead to immediate labour, it is not recommended when the need to get the baby out is urgent. Its primary use is to “prevent” a longer gestation and therefore an induction by more risky means.
A stretch-and-sweep is a procedure that is meant to induce labour so that you won’t be induced later. The Society of Obstetricians and Gynaecologists of Canada wrote in their 2013 Practice Guideline, which was reaffirmed in 2015, that “routine sweeping (stripping) of membranes promotes the onset of labour and that this simple technique decreases induction rates.”
Again: membrane sweeping is a procedure meant to induce labour so that the client won’t be induced later.
It assumes that the later induction is non-negotiable and the client’s best hope is that this early induction “saves” her from the risks of the later induction.
This is no different than all those “natural” inductions that are employed when trying to induce labour so the mother doesn’t have experience an induction – or the challenge of just declining the planned induction. It takes the approach that planned inductions are non-negotiable. Of course, mothers may chose a natural induction as a means of expediting the births of their babies for a number of reasons and I fully support their autonomy and choice to do so.
If there is a medical need to get the baby out to preserve its or its mothers life, then this dyad should be under medical supervision and receiving the best medical care possible. We need to critically evaluate the mentality that says, “let’s try to induce so we don’t have to induce”.
We’ve bought into a culture where non-evidence-based time limits and spurious reasons are given for booking inductions that don’t line up with the science. Rather than supporting mothers in exploring the science, doing a targeted risk/benefit analysis based on her particular situation, and supporting the mother in informed decision making, we line up the early inductions hoping to out-smart, out-wit, and out-play the medical providers who routinely induce based on outdated information or habit or hospital protocols that are based in their insurance risk-management strategy.
If this procedure is not recommended when there is an urgent need to get the baby out (Bouvain et al., 2005) and its primary purpose is to prevent a later induction where the indication is a pregnancy continuing beyond the cut-off date of the caregiver or institution (SOGC, 2013), then it has no medical indication.
What else did the Cochrane Review find?
There was a high level of bias in many of the studies, in part, because there could be no blinding. The clinicians knew they were performing the procedure and the clients knew they’d received it due to discomfort and pain
It was an out-patient procedure meaning there was no urgent reason for the induction
It did not generally lead to labour within 24 hours
No difference in oxytocin augmentation, use of epidural, instrumental delivery, caesarean delivery, meconium staining, admission to the NICU, or Apgar score less than seven at five minutes between sweeping and non-sweeping. This means it didn’t show any benefit
No difference in pre-labour rupture of membranes, maternal infection or neonatal infection. However, it’s worth noting that the non-sweeping participants were subject to routine obstetrical services that includes many vaginal exams that increase pre-labour rupture of membranes and infection (Maharaj, 2007; Zanella et al., 2010; Lenihan, 1984; Critchfield et al., 2013)
Significant pain in the mother during the procedure
Vaginal bleeding after the procedure
Painful contractions for the next 24 hours not leading to labour
What we have here is a routine that hurts the mother and has no significant benefit – aside from maybe possibly putting her into labour before another planned induction.
As the Cochrane Review discovered, the likely outcome of a membrane sweep is painful non-progressing contractions. This is often mis-interpreted as “labour” and the client is sent to the hospital for an induction anyway because she’s been “in labour” for 24-48 hours without progress. This is the epitome of a hijacked birth that turns a normal physiological process into a pathological one leading to the cascade of interventions, sometimes all the way up to an unwanted and unplanned caesarean for “failure to progress”. To convert the natural process into a pathological one is part of the classic definition of obstetrical violence (D'Gregorio, 2010).
They call it ‘birth rape’
For those who experienced this without their prior knowledge or consent, their comments overwhelmingly spoke of rape. This was especially pronounced in those with a history of prior rape. Studies confirm that those with a history of rape experience the routines of industrial birth differently than those without a history of sexual assault. For survivors, procedures that are uneventful for others can inadvertently put them “back in the rape” (Halvorsen, Nerum, Øian, & Sørlie, 2013).
Frankly, it’s unconscionable that any care provider would brazenly take the opportunity to manually manipulate a woman’s cervix, knowing it introduces risks and has the potential to hurt her, without the express knowledge and consent of the client following an informed choice discussion.
While membrane sweeping is intended to induce labour, it’s also used on labouring women to hurry things along. During labour, the cervix is being moved and thinned by the action of uterine muscles contracting and pulling the cervix up and around the baby’s head. The cervix is working hard and it’s tender. Many women will report that they screamed, cried ‘no’, tried to kick the provider’s hand away, or tried to crawl up the bed to get away from the invasive exam.
I remember one dark cold February night, years ago, when I was called to be with a family in labour. There was an ice storm and my trip there was dangerous and precarious. Eventually, my car slid into their street and managed to stop somewhere close to the driveway. I quietly entered the house to hear a mother in the throes of glorious, deep, active labour. I knew it wouldn’t be long before the baby arrived. I announced myself and tiptoed upstairs to see her on hands and knees with more blood than I would have expected on the towel beneath her. She said she invited her midwife to the birth and expected her to be there any minute. Soon enough, a beautiful baby boy gently emerged and landed safely into his daddy’s waiting hands. By the time the midwives arrived, the new family was tucked into bed enjoying a post-birth snack and cup of tea.
As the new family was bonding, I joined the midwives downstairs who were making notes in their client’s medical charts to make them some tea and offer a snack. I overheard one midwife say, “Oh yeah, when I was here earlier, she was about 6cm so I did a stretch-and-sweep”.
“Oh yeah.
Now I remember.
She was in active labour so I did an invasive and painful procedure to speed things up during a dark and dangerous ice storm.
Without her knowing I would do that.”
This is nothing but reckless cruelty. Yet this kind of cruelty permeates maternity services where women are routinely hurt for the sole purpose of interfering in their physiology and the safety of the birth process in order to get the baby out before they do even more risky and dangerous things.
And that is why I would like to see the ROUTINE, WITHOUT MEDICAL INDICATION membrane sweep removed from obstetrical and midwifery practice. It shouldn’t be the luck of the draw that a pregnant client gets one of the “good ones” who only induces a client when there is a medical need, with an informed choice discussion, and full consent.
To return to my original question: what is it about membrane sweeping that is so cherished that challenging it generates death threats?
It’s a deeply embedded ritual in a toxic medical culture that presumes to take authority over a pregnant woman’s sexual organs for the purpose of dominating the physiological process and then becoming a hero to the interrupted physiology and complications that ensue. It’s about power and control. And challenging this is a dangerous act of sedition. Those who do this to their clients like being the hero and clients who defend this need to believe they were saved from something – otherwise the truth is just too awful.
Make wise choices.
Much love,
Mother Billie
#endobstetricalnonsense #informedconsent #obstetricalviolence #membranesweeping #stretchandsweep #withoutconsent #birthrape #failuretoprogress
References
Better Outcomes Registry Network. (BORN). 2013. Provincial Overview of Perinatal Health in 2011–2012.
Boulvain, M., Stan, C. M., & Irion, O. (2005). Membrane sweeping for induction of labour. Cochrane Database of Systematic Reviews, (1).
Buckley, S. J. (2015). Hormonal physiology of childbearing: Evidence and implications for women, babies, and maternity care. Washington, DC: Childbirth Connection Programs, National Partnership for Women & Families.
Cohain, J. S. Reducing Inductions: Lack of Justification to Induce for “Postdates”.
Critchfield, A. S., Yao, G., Jaishankar, A., Friedlander, R. S., Lieleg, O., Doyle, P. S., ... & Ribbeck, K. (2013). Cervical mucus properties stratify risk for preterm birth. PloS one, 8(8), e69528.
D'Gregorio, R. P. (2010). Obstetric violence: a new legal term introduced in Venezuela.
Halvorsen, L., Nerum, H., Øian, P., & Sørlie, T. (2013). Giving birth with rape in one's past: a qualitative study. Birth, 40(3), 182-191.
King, V., Pilliod, R., & Little, A. (2010). Rapid review: Elective induction of labor. Portland: Center for Evidence-based Policy.
Lenihan, J. J. (1984). Relationship of antepartum pelvic examinations to premature rupture of the membranes. Obstetrics and gynecology, 63(1), 33-37.
Leppert, P. C. (1995). Anatomy and physiology of cervical ripening. Clinical obstetrics and gynecology, 38(2), 267-279.
Maharaj, D. (2007). Puerperal pyrexia: a review. Part II. Obstetrical & gynecological survey, 62(6), 400-406.
Mandruzzato, G., Alfirevic, Z., Chervenak, F., Gruenebaum, A., Heimstad, R., Heinonen, S., ... & Thilaganathan, B. (2010). Guidelines for the management of postterm pregnancy. Journal of perinatal medicine, 38(2), 111-119.
Mozurkewich, E., Chilimigras, J., Koepke, E., Keeton, K., & King, V. J. (2009). Indications for induction of labour: a best‐evidence review. BJOG: An International Journal of Obstetrics & Gynaecology, 116(5), 626-636.
Osterman, M. J., & Martin, J. A. (2014). Recent declines in induction of labor by gestational age.
Rao, A., Celik, E., Poggi, S., Poon, L., & Nicolaides, K. H. (2008). Cervical length and maternal factors in expectantly managed prolonged pregnancy: prediction of onset of labor and mode of delivery. Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 32(5), 646-65.
Rayburn, W. F., & Zhang, J. (2002). Rising rates of labor induction: present concerns and future strategies. Obstetrics & gynecology, 100(1), 164-167.
Society of Obstetricians and Gynaecologists of Canada. SOGC. 2013. Clinical Practice Guideline, No. 296, Indution of Labour.
Tan, P. C., Khine, P. P., Sabdin, N. H., Vallikkannu, N., & Sulaiman, S. (2011). Effect of membrane sweeping on cervical length by transvaginal ultrasonography and impact of cervical shortening on cesarean delivery. Journal of Ultrasound in Medicine, 30(2), 227-233.
Zanella, P., Bogana, G., Ciullo, R., Zambon, A., Serena, A., & Albertin, M. A. (2010). Chorioamnionitis in the delivery room. Minerva pediatrica, 62(3 Suppl 1), 151-153.
On the Art of Discussing Paradigm-Shifting Topics
Everyone has an intellectual/mental/emotional operating system – a personal paradigm that serves as a frame of reference containing basic assumptions and ways of thinking. This personal paradigm is the means by which we make sense of the world around us. It helps us to filter, understand, and categorise information and experiences. It helps us to know what is “true” and what isn’t; it guides our responses and our actions.
Humans are designed to be in connection with each other. We operate mostly unconsciously through hormones, synapses, and other magical pathways. Our primary operating system is our para-sympathetic nervous system – our “calm and connected” system. This part of our autonomic nervous system keeps our hearts beating, our lungs breathing, and our food digesting. The main hormone of this system is oxytocin – the hormone of love, trust, bonding, and connection. This is why isolation is so effective at crushing and changing people, and why friends and loved ones can heal and nurture new ideas.
Personal paradigms, once settled and serving us reasonably well are most likely to be changed by 2 things: Great Suffering or Great Love.
Everyone has an intellectual/mental/emotional operating system – a personal paradigm that serves as a frame of reference containing basic assumptions and ways of thinking. This personal paradigm is the means by which we make sense of the world around us. It helps us to filter, understand, and categorise information and experiences. It helps us to know what is “true” and what isn’t; it guides our responses and our actions.

Source: Paradigm Dramas in American Studies: A Cultural and Institutional History of the Movement. Gene Wise American Quarterly, Volume 31:3 (1979): 293-337.
For someone who was raised on the streets, relying on street-smarts and their wits, they may understand the world to be a hostile place with scarce resources and easily manipulated marks. This guides their responses and their actions. However, someone raised in a loving home with abundance and gentle guidance may understand the world to be an accommodating place where hard work and relationships lead to prosperity and contentment.
A personal paradigm develops over one’s lifetime and depends on many things,
One’s macro-culture – that’s the big stuff, like country of origin, current community, heritage, race, and cultural history
One’s micro-culture – that’s the smaller stuff, like family of origin, friends, current family members, or caregivers
Education – this includes the schools one attended, what was learnt, whether they felt successful in their education, and how the individual has continued to educate themselves, including interacting with mentors
Personal experiences – this is the stuff one has experienced in their lifetime and what it’s taught them about themselves, others, and the world around them
Media – the movies that are viewed, the stories read, the news that’s told, the images shown, the podcasts listened to, and the pages and the people followed
This is how we make sense of the world.
When someone is told that they are part of the privileged, they’re going to evaluate that against their personal paradigm, in particular, their personal experiences. They’ll be thinking of whether they were sent to school or educated. Whether they had enough food each day or a safe home to live in. Whether they were beat up or molested in childhood or how many important people in their life died. Or how many times they’ve been sexually assaulted. They may not feel particularly privileged.
Likewise, an individual whose life is filled with opportunity and meaningful relationships may not feel marginalised, despite sharing some characteristics or heritage with traditionally marginalised groups.
An individual with a background rife with adverse childhood experiences loses the perspective that theirs is a life of privilege when compared to those who are denied even more basic human rights due to race, ethnicity, gender, orientation, or heritage. Without connection with others against which to juxtapose their experiences, they are unlikely to understand the meaning of their privilege. Understanding comes through compassionate connection with those whose lives are different and with mentors who can lead the way.
Humans are designed to be in connection with each other. We operate mostly unconsciously through hormones, synapses, and other magical pathways. Our primary operating system is our para-sympathetic nervous system – our “calm and connected” system. This part of our autonomic nervous system keeps our hearts beating, our lungs breathing, and our food digesting. The main hormone of this system is oxytocin – the hormone of love, trust, bonding, and connection. This is why isolation is so effective at crushing and changing people, and why friends and loved ones can heal and nurture new ideas.
Personal paradigms, once settled and serving us reasonably well are most likely to be changed by 2 things: Great Suffering or Great Love.
Since I work in trauma, I see how Great Suffering rips out the core of an individual and changes their very identity, their very essence. And I see how Great Love can bring healing, restoration, a new way of viewing themselves and others, and a new way of interacting in the world.
When engaging in paradigm shifting conversations, such as privilege, racism, cultural appropriation, medical routines, consumerism, religion & faith, parenting, etc., there are a few things to consider:
What is your motive for engaging in the conversation?
Are you hoping to change the other person’s perspective? In this case, you’ll have to consider if you’ll employ Great Suffering or Great Love.
Will your conversation foster human connection?
Will everyone emerge from the conversation grateful for having been a part of it?
The key to engaging in a conversation that fosters human connection, and therefore, the opportunity to encourage paradigm-shifting changes, is empathy.
Empathy is the art of considering something from the other’s vantage, i.e. wearing their shoes (metaphorically) for a mile. It is connecting by establishing emotional resonance with the other person by placing oneself in their situation and looking through their eyes. Empathy is other-centred.
Sympathy is the art of considering something from our own vantage, by drawing upon our own experiences and feelings in order to connect through a shared or common experience or history. It is connection by looking inward in order to establish a common or shared experience. Sympathy is self-centred.

Empathy is the glue that holds us together as humans sharing life on this planet together. When I’m talking about paradigm-shifting conversations, I’m talking about communication between two or more reasonable people. This does not include narcissists or sociopaths. I’m also not talking about advocacy.
Lack of empathy is a defining characteristic of narcissists and sociopaths and they are generally impervious to connection based on achieving emotional resonance or to changing their perspective based on another’s suffering. It’s probably an exercise in futility to attempt to converse in paradigm-challenging topics.
Advocacy is a form of communication that elevates the voice(s) of those who are not being heard or are unable to speak for themselves. It seeks to ensure the voices of those who are disadvantaged, marginalised, oppressed, hurt, or excluded are represented. Their voices may be angry, frustrated, grieving, incensed, or frightened. Advocacy does not target an individual for reciprocal oppression, but rather brings awareness about systems and structures that permit individuals to oppress, hurt, exclude, and marginalise others. Advocacy opens eyes and brings people to the table to talk where empathy connects individuals. Connection, built on empathy, changes individuals who then leave oppressive systems and abandon marginalising behaviours to become agents of change and advocates.
Dominant cultures and dominant paradigms do not need to advocate for their own perspective. It is unnecessary to elevate their own voices or to engage in mockery, derision, denigration, or social isolation for the few that disagree with them.

unsplash.com
If we take today’s near hysteria regarding vaccines, how many families who no longer vaccinate their children, for whatever reason, including death or injury of a previously vaccinated child, moral objection to ingredients, scientific investigation, etc., have changed their minds as a result of having their children called “crotch fruit”, or being told they are too stupid to know vaccines save lives, that the lives of their children should be left to the professionals, or that they should be arrested and have their children taken from them? I’ll go out on a limb here and say “none”. Perhaps it’s a good example of how mockery, bullying, and denigration from a dominant group is more about bonding to their own kind than actually changing someone else’s perspective.
Personal paradigms are deeply entrenched operating systems. They don’t change because someone says we are wrong or someone says we are hurting others. Where advocacy opens eyes, empathy reaches deep into our limbic system where cherished beliefs are held. Empathy disarms fear; connection heals emotional wounds.
My paradigm-shifting changes happened because I was in connection with people who cared. They validated my concerns and shared their lives with me. I am changing my perspective on many things today because of deep connections that include mutual validation, concern, and love. I would no more want to hurt someone I care about by my thoughts or actions than I want to be hurt by another’s.
As privileged and marginalised peoples, we will only learn to connect in shared human experiences as members of this planet when we connect in love and empathy.
Paradigm-shifting conversations between two or more reasonable people begin with empathy for everyone’s learned experience, whether we’re talking about racism, privilege, cultural appropriation, marginalisation, consumerism, global warming, vaccinations, obstetrical violence, birth trauma, or veganism. Life has been tough for far too many people so far. Proceed with care.
Much love,
Mother Billie

unsplash.com
Birthing after Trauma – Seeing the Bigger Picture
It’s frustrating for care providers when their client comes armed with a 10-page birth plan, an army of doulas, and a mistrustful and hostile attitude. Care providers exist for the sole purpose of providing medical or midwifery services for pregnant, birthing, and postpartum clients and their goal is to help them emerge healthy and whole. Unfortunately, this creates friction before the relationship begins.
A mistrustful client has probably already had her trust broken by someone else long before they come armed with the minute details of how they need things to unfold. They may have already experienced abuse, neglect, sexual assault, victimisation, and trauma. Their trauma might have been the result of an abusive childhood, racial adversity, marginalisation, being the victim of a crime, or it might have been the result of a previous traumatic birth experience.
Published on Birth Trauma Ontario November 11, 2018
It Begins with a Mistrustful Client

Photo Martin Walls freeimages.com
It’s frustrating for care providers when their client comes armed with a 10-page birth plan, an army of doulas, and a mistrustful and hostile attitude. Care providers exist for the sole purpose of providing medical or midwifery services for pregnant, birthing, and postpartum clients and their goal is to help them emerge healthy and whole. Unfortunately, this creates friction before the relationship begins.
A mistrustful client has probably already had her trust broken by someone else long before they come armed with the minute details of how they need things to unfold. They may have already experienced abuse, neglect, sexual assault, victimisation, and trauma. Their trauma might have been the result of an abusive childhood, racial adversity, marginalisation, being the victim of a crime, or it might have been the result of a previous traumatic birth experience.
Birth Trauma Changes the Individual
Birth trauma doesn’t just happen. It’s not connected to an emergency or an unexpected outcome. These parents are not looking for someone to blame. Birth trauma is the result of clearly defined factors where the greatest indicator is a breakdown in the relationship between the care providers and the client (Harris & Ayers, 2012). The birthing mother felt disrespected, lied to, coerced, bullied, ignored, unsupported, and like she was just another cog in the wheel (Beck 2004; Reed, Reed, Sharman & Inglis, 2017). When this is partnered with pre-existing risk factors, this individual is at risk for developing postpartum post-traumatic stress disorder (Wu, Molteni, Ying, & Gomez-Pinilla, 2003; Faravelli, Giugni, Salvatori, & Ricca, 2004; Fromm, Heath, Vink, & Nimmo, 2004; Cortina &Kubiak, 2006; Eby & Eby, 2006; Sarandol et al., 2007; Lev-Wiesel, Chen, Daphna-Tekoah, & Hod, 2009; Roberts, Austin, Corliss, Vandermorris, & Koenen, 2010; Beck, Gable, Sakala, & Declercq, 2011; Cisternas et al., 2015; Matsumura et al., 2016; Du et al., 2016).
When parents have had a traumatic birth (about one third of all parents), they are much less likely to have another child, even if they wanted a larger family. In fact, they are twice as likely to not have another baby as someone who had a positive experience. If they choose to have another baby, the spacing between babies is twice as long as someone who had a positive experience. It takes them a much longer time to work up to doing it again (Gottvall & Waldenström, 2002).
Birthing after a traumatic experience is very different than preparing to birth a first child or another baby after a positive experience. These mothers are likely still dealing with the symptoms of trauma – flashbacks, sleep disturbances, terror, rage, difficulty forming new memories, hyperarousal always being on guard, and avoidance of triggers – including care providers and hospitals. These mothers are also more likely to be dealing with depression, anxiety, changes in their functional capacity, and suicidal thoughts than mothers without trauma. (DSM-5, 2013; Brady, Killeen, Brewerton, & Lucerini, 2000; Cook et al., 2004; Tavares et al., 2012).
When a Parent-of-Trauma Gets Pregnant Again
When a woman has had a traumatic birth and may still be suffering the effects of trauma, a new pregnancy can be a profoundly challenging time for her. She must now come face-to-face with the possibility that she will possibly endure the same horror in order to welcome this child into the world. Feelings of desperation, despair, fear, terror, and suicidal thoughts are not uncommon. Thoughts of running away and birthing alone in the woods are also common. This dread often interferes with bonding to her baby. (Beck & Watson, 2010)
The healthcare and birthing choices these parents make for subsequent births can be quite varied and diverse. Some might choose the same provider and location simply because it’s familiar and they know what’s coming. They know that they survived it the first time, and therefore can survive it again.
They might plan a caesarean section to gain the most control over the event. This way they can choose the surgeon, the day, and their support team. They won’t be facing the unknowns of whichever provider is on call.
If a mother chooses a vaginal birth, its very common for them to hire a doula as an advocate, to change providers, hospitals, plan a homebirth, or even birth in another city.
Unassisted Birth Choices

Freebirth, unassisted birth, or family birth, where there is no licensed medical attendant present, is a choice that is appearing more frequently in many developed countries (Holton & de Miranda, 2016). It’s a choice that is more common among parents who are birthing after trauma. Unassisted birth choices speak to the resistance that can be a response to the biomedical model of birth. Some families are finding that the obstetrical and midwifery model of risk-aversion and risk management removes their autonomy, and violates their culture, values, faith, or at times, their sexuality. If a mother has received disrespectful care, then they are more likely to avoid these services for subsequent pregnancies (UNPA, 2004). In an online survey of families that chose an unassisted birth, over half identified a previous negative hospital experience as the reason for their choice (O’Day, 2016). While there is no licensed medical attendant present, an unassisted birth may include the support of family members, doulas, traditional birth attendants, or other companions.
No matter what the mother-of-trauma chooses, she is disadvantaged because she can’t control for the behaviour of others in the medical system that don’t understand or respect her trauma or her perspective. Even the mother who chooses an unassisted birth may still be persecuted by hostile services if she transfers to the hospital for medical care (Vedam et al., 2017). Many a mother seeking medical support is “welcomed” by a harassing call to child protective services to investigate whether she is “conforming” to conventional medical services (Diaz-Tello, 2016). Online forums are filled with discussions on how to manage a possible trip to the hospital or doctor and how to prepare for a potentially harassing call to Childrens Aid Society (CAS), including sharing contact information for advocates and legal services. Indeed, misinformed providers are participating in this spiraling disconnect between clients and needed healthcare services.
Inappropriate Responses to Unconventional Choices
Providers will note that some of their clients decline the usual suite of obstetrical or midwifery services. For some clients, it’s an evidence-based decision. And for others, they are trying to avoid triggering their symptoms of trauma (Beck & Watson, 2010). Again, ill-equipped providers have been known to report these mothers to CAS, thinking that their health care choices are dangerous to the fetus. These are potentially well-meaning individuals, but have violated their professional ethics, as they cannot induce duress, bullying, or coercion to gain compliance (Health Care Consent Act, 1996). Further, the fetus has no citizenship and investigation by CAS regarding a fetus would be tantamount to harassment. However, this is one more obstacle that mothers-of-trauma often must navigate as they disentangle themselves from disrespectful care.
The consequence of these inappropriate actions from care providers is that mothers-of trauma will often decline further medical services for their babies once they are born, or to seek follow-up care or breastfeeding support (Finlayson & Downe, 2013; Moyer, Adongo, Aborigo, Hodgson, & Engmann, 2014). While pregnant, they may lie about their plans, their health, and other pertinent information, thereby missing an opportunity to form a collaborative relationship that could build lifetime wellness and resilience. They may choose to birth their babies without assistance and then tell their care provider that it just happened “too quickly”. This is ongoing evidence of the breakdown in the relationship between client and clinician.
Where Doulas Can Help
Doulas are the client’s and the clinician’s greatest ally as they generally develop the trust of the pregnant family and offer to serve as their advocate. Doulas can have a significant impact on the client’s outcome by reducing the need for surgery, assisted delivery, analgesia, and contributing to the reduction in low Apgars for the baby, and postpartum depression for the mother (Bohren, Hofmeyr, Sakala, Fukuzawa, & Cuthbert, 2017). Without the risk of reporting a non-compliant client, it is the doula that is privy to the client’s previous traumatic experience, the client’s coping strategies, and the wellbeing of the family. The doula has the opportunity to connect the client to resources in their community or to serve as a companion at medical visits. The rise of the doula to support families is indicative of a system that routinely denies birthing individuals informed choice, dignified care, and trauma-informed care (Dahlen, Jackson, & Stevens, 2011). Unfortunately, the burnout rate for doulas is very high due to vicarious trauma and institutional hostility (Naiman-Sessions, Henley, & Roth, 2017), meaning that experienced doulas are hard to find and it’s nearly impossible to foster their growth within the current medical paradigm.

© Billie Harrigan Consulting
Preparing to Birth After Trauma
When preparing to birth after trauma, the pregnant mother will often engage in a number of strategies that might seem excessive to someone who had a positive experience or to the provider who is not trauma-informed (Beck & Watson, 2010; Harrigan, 2017). These strategies can include:
Detailed, extensive, and lengthy birth plans
Hiring a doula
Doing extensive research into providers, locations, routines, and unassisted birth
Avoiding the usual suite of maternity services, such as ultrasound or scheduled prenatal visits
Doing birth art
Writing positive affirmations
Choosing complementary medicine to address health issues
Joining with other parents to learn more about birth, including how to have a breech baby, neonatal resuscitation, pre-eclampsia, etc.
Birth Plans – A Trauma Narrative in Disguise

Lengthy birth plans are generally the client’s attempt at communicating with their care team. It often represents their trauma narrative and is the care provider’s window into their client’s suffering that has brought them to this place. As a form of communication, however, it’s quite ineffective as far too many institutional cultures regard the birth plan as a joke where the longer the birth plan, the sooner she’s booked into the OR for a caesarean. Further, it has no impact on the care provider’s behaviour towards the client and may increase the client’s negative feelings about their birth (Berg, Lundgren, & Lindmark, 2003).
The client-of-trauma is again disadvantaged in trying to garner empathetic care in light of institutional hostility towards various modes of communication, including a birth plan, the use of a doula, self-advocacy, or the inclusion of other advocates. Attempts on the part of the client to change institutional culture are wholly ineffective if the entire facility isn’t addressing entrenched biases (Betrán et al., 2018).
It Begins with an Empathetic Trauma-Informed Care Provider

Photo credit: http://www.thefirsthelloproject.com
Birthing after trauma sometimes feels like a herculean feat for the mother where she is taken on a roller coaster of fear, despair, opposition, obstacles, institutional hostility, ill-equipped care providers, and unfortunately thoughts of suicide.
Yet, there is great hope. As more care providers become trauma-informed and institutions develop appropriate practices to support the client-of-trauma and develop a collaborative and respectful culture, the client can emerge with greater wellness, increased resilience, and growing trust. When a woman has a subsequent birth that fuels her post-traumatic growth, she credits the caring support of her care providers as a crucial element (Beck, 2010)
Nothing compares to the gift of a healing care provider.
Much love,
Mother Billie
References:
Beck, C. T. (2004). Birth trauma: in the eye of the beholder. Nursing Research, 53(1), 28-35.
Beck, C. T., & Watson, S. (2010). Subsequent childbirth after a previous traumatic birth. Nursing research, 59(4), 241-249.
Beck, C. T., Gable, R. K., Sakala, C., & Declercq, E. R. (2011). Posttraumatic stress disorder in new mothers: Results from a two‐stage US National Survey. Birth, 38(3), 216-227.
Berg, M., Lundgren, I., Lindmark G. (2003). Childbirth experience in women at risk: Is it improved by a birth plan? Journal of Perinatal Education. 12(2):1–15.
Betrán, A. P., Temmerman, M., Kingdon, C., Mohiddin, A., Opiyo, N., Torloni, M. R., ... & Downe, S. (2018). Interventions to reduce unnecessary caesarean sections in healthy women and babies. The Lancet, 392(10155), 1358-1368.
Bohren, M. A., Hofmeyr, G. J., Sakala, C., Fukuzawa, R. K., & Cuthbert, A. (2017). Continuous support for women during childbirth. The Cochrane Library.
Brady, K. T., Killeen, T. K., Brewerton, T., & Lucerini, S. (2000). Comorbidity of psychiatric disorders and posttraumatic stress disorder. Journal of Clinical Psychiatry,61, 22-32.
Cisternas, P., Salazar, P., Serrano, F. G., Montecinos-Oliva, C., Arredondo, S. B., Varela-Nallar, L., ... & Inestrosa, N. C. (2015). Fructose consumption reduces hippocampal synaptic plasticity underlying cognitive performance. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease,1852(11), 2379-2390.
Cortina, L. M., & Kubiak, S. P. (2006). Gender and posttraumatic stress: sexual violence as an explanation for women's increased risk. Journal of abnormal psychology, 115(4), 753.
Cook, C. A. L., Flick, L. H., Homan, S. M., Campbell, C., McSweeney, M., & Gallagher, M. E. (2004). Posttraumatic stress disorder in pregnancy: prevalence, risk factors, and treatment. Obstetrics & Gynecology, 103(4), 710-717.
Coxon, K., Homer, C., Bisits, A., Sandall, J., & Bick, D. (2016). Reconceptualising risk in childbirth. Midwifery, 38, 1-5.
Dahlen, H. G., Jackson, M., & Stevens, J. (2011). Homebirth, freebirth and doulas: casualty and consequences of a broken maternity system. Women and Birth, 24(1), 47-50.
Diagnostic and Statistical Manual of Mental Disorders (DSM-5) American Psychiatric Assoc Pub; 5 edition(May 22 2013).
Diaz-Tello, F. (2016). Invisible wounds: obstetric violence in the United States. Reproductive Health Matters.
Du, J., Zhu, M., Bao, H., Li, B., Dong, Y., Xiao, C., ... & Vitiello, B. (2016). The role of nutrients in protecting mitochondrial function and neurotransmitter signaling: implications for the treatment of depression, PTSD, and suicidal behaviors. Critical reviews in food science and nutrition, 56(15), 2560-2578.
Eby, G. A., & Eby, K. L. (2006). Rapid recovery from major depression using magnesium treatment. Medical hypotheses, 67(2), 362-370.
Faravelli, C., Giugni, A., Salvatori, S., & Ricca, V. (2004). Psychopathology after rape. American Journal of Psychiatry, 161(8), 1483-1485.
Finlayson, K., & Downe, S. (2013). Why do women not use antenatal services in low-and middle-income countries? A meta-synthesis of qualitative studies. PLoS medicine, 10(1), e1001373.
Fromm, L., Heath, D. L., Vink, R., & Nimmo, A. J. (2004). Magnesium attenuates post-traumatic depression/anxiety following diffuse traumatic brain injury in rats. Journal of the American College of Nutrition, 23(5), 529S-533S.
Gottvall, K., & Waldenström, U. (2002). Does a traumatic birth experience have an impact on future reproduction?. BJOG: An International Journal of Obstetrics & Gynaecology,109(3), 254-260.
Harrigan, Billie. (2017). The Epic Failure of the Evidence-Based Movement. https://www.billieharrigan.com/blog/2017/1/16/the-epic-failure-of-the-evidence-based-movement.
Harris, R., & Ayers, S. (2012). What makes labour and birth traumatic? A survey of intrapartum ‘hotspots’. Psychology & Health, 27(10), 1166-1177.
Health Care Consent Act, 1996, S.O. 1996, c. 2, Sched. A
Holten, L., & de Miranda, E. (2016). Women׳s motivations for having unassisted childbirth or high-risk homebirth: An exploration of the literature on ‘birthing outside the system’. Midwifery.
Lev-Wiesel, R., Chen, R., Daphna-Tekoah, S., & Hod, M. (2009). Past traumatic events: are they a risk factor for high-risk pregnancy, delivery complications, and postpartum posttraumatic symptoms?. Journal of Women's Health, 18(1), 119-125.
Matsumura, K., Noguchi, H., Nishi, D., Hamazaki, K., Hamazaki, T., & Matsuoka, Y. J. (2016). Effects of omega-3 polyunsaturated fatty acids on psychophysiological symptoms of post-traumatic stress disorder in accident survivors: a randomized, double-blind, placebo-controlled trial. Journal of affective disorders.
Moyer, C. A., Adongo, P. B., Aborigo, R. A., Hodgson, A., & Engmann, C. M. (2014). ‘They treat you like you are not a human being’: maltreatment during labour and delivery in rural northern Ghana. Midwifery, 30(2), 262-268.
Naiman-Sessions, M., Henley, M. M., & Roth, L. M. (2017). Bearing the Burden of Care: Emotional Burnout Among Maternity Support Workers. In Health and Health Care Concerns Among Women and Racial and Ethnic Minorities (pp. 99-125). Emerald Publishing Limited.
O’Day, Katharine, L, "Outside the System": Motivations and Outcomes of Unassisted Childbirth. Transitions Midwifery Institute, Published online November 19, 2016.
Reed, R., Sharman, R., & Inglis, C. (2017). Women’s descriptions of childbirth trauma relating to care provider actions and interactions. BMC pregnancy and childbirth, 17(1), 21.
Roberts, A. L., Austin, S. B., Corliss, H. L., Vandermorris, A. K., & Koenen, K. C. (2010). Pervasive trauma exposure among US sexual orientation minority adults and risk of posttraumatic stress disorder. American Journal of Public Health, 100(12), 2433-2441.
Sarandol, A., Sarandol, E., Eker, S. S., Erdinc, S., Vatansever, E., & Kirli, S. (2007). Major depressive disorder is accompanied with oxidative stress: short‐term antidepressant treatment does not alter oxidative–antioxidative systems. Human Psychopharmacology: Clinical and Experimental, 22(2), 67-73.
Tavares, D., Quevedo, L., Jansen, K., Souza, L., Pinheiro, R., & Silva, R. (2012). Prevalence of suicide risk and comorbidities in postpartum women in Pelotas. Revista Brasileira de Psiquiatria, 34(3), 270-276.
United Nations Population Fund. (2004) in: UNFPA (Ed.) State of the World Population 2004. UNFPA, New York.
Vedam, S., Stoll, K., Rubashkin, N., Martin, K., Miller-Vedam, Z., Hayes-Klein, H., & Jolicoeur, G. (2017). The mothers on respect (MOR) index: measuring quality, safety, and human rights in childbirth. SSM-population health, 3, 201-210.
Wu, A., Molteni, R., Ying, Z., & Gomez-Pinilla, F. (2003). A saturated-fat diet aggravates the outcome of traumatic brain injury on hippocampal plasticity and cognitive function by reducing brain-derived neurotrophic factor. Neuroscience, 119(2), 365-375.
When not to induce – reason #408 – a placenta with calcium deposits
I received yet another phone call from someone who was trying to sort out the risks of staying pregnant versus the risks of being induced. From what the client could share, it was hard to know if the practitioner wasn’t fully informed on placental calcification at term, or wasn’t fully forthcoming about the non-clinical indications of that particular development in a healthy pregnancy.
To be sure, there are times when the benefits of an induction to rescue a compromised baby far outweigh the short and long-term risks of an induction.
Unfortunately, when trying to make an informed decision, clients often need to learn what their practitioners don’t know or won’t tell them.
“I’m 3 days overdue and my midwife says I need to be induced because my placenta is calcifying and that means it’s dying.”

I received yet another phone call from someone who was trying to sort out the risks of staying pregnant versus the risks of being induced. From what the client could share, it was hard to know if the practitioner wasn’t fully informed on placental calcification at term, or wasn’t fully forthcoming about the non-clinical indications of that particular development in a healthy pregnancy.
To be sure, there are times when the benefits of an induction to rescue a compromised baby far outweigh the short and long-term risks of an induction.
Unfortunately, when trying to make an informed decision, clients often need to learn what their practitioners don’t know or won’t tell them. So let’s take a little tour of the placenta.

© Billie Harrigan Consulting
To begin, the placenta is a fetal organ, meaning it is made from the same sperm and egg that makes the baby. As the baby grows and ages, so does the placenta. Both the baby and the placenta (which comes from the same genetic material) need to reach a certain level of maturity in order to be born healthy. The placenta does not suddenly expire when the pregnancy reaches an arbitrary number of weeks.
When the placenta is not well, the baby is usually not well. When the baby is well, then the placenta is usually well. Sometimes, there are variations in the placenta that are more common in babies at risk and they might also be present in a healthy baby. So not all variations mean something is wrong every time.
The placenta is a marvellous organ that has a maternal side that attaches to the wall of the mother’s uterus, and a fetal side where the umbilical cord arises to transport blood back and forth from the fetus to the placenta.
The umbilical cord usually has 2 arteries (going away from the baby’s heart towards the placenta) and one vein (returning back to the baby’s heart). So while blood that is full of oxygen is usually flowing through our arteries, in the case of the umbilical arteries, it’s going away from the baby to the placenta with waste and then the umbilical vein returns to the heart with oxygen and nutrients that are supplied by the placenta. The surrounding Wharton’s Jelly protects these important vessels inside the cord.
The mother’s blood and the baby’s blood don’t intermingle thanks to the wisdom of the placenta and the uterus working together. However, the baby gets all it’s nutrients from the mother’s blood stream and counts on mum to clean the waste the baby produces. Thanks to something called trophoblasts, which extend from the placenta into an area of the uterus where mum’s blood flows freely, oxygen and carbon dioxide and various nutrients and wastes are exchanged between mum and baby without baby’s blood and mum’s blood touching each other.
Khan Academy – meet the placenta
Due to the wonders of ultrasound, we’re now taking a look at things that were once hidden. And since we love to organise what we see and give things names, the placenta has been given names to indicate where it is in its development, as seen through ultrasounds:
Grade 0: less than 18 weeks gestation
Grade I: 18-29 weeks gestation
Grade II: 30-38 weeks gestation
Grade III: 39 weeks until birth
Each of these “grades” has specific features that help the technician to “date” the placenta.
One of the features of a Grade III placenta is that it often shows circular indentations that have calcium deposits (calcification). This is considered to be a natural part of the aging process in much the same way that our skin develops wrinkles as we age. And just as wrinkles in the skin of a person of any age doesn’t mean that this person is at risk of imminent death, neither does the appearance of calcification in a normal placenta at term mean that it’s about to expire (Harris & Alexander, 2000; Jamal et al., 2017; Nolan, 1998).
So where did this idea come from that calcification on a placenta meant it was dying?
This notion has come from the observation and study of preterm births of compromised fetuses. A compromised fetus that is born early often has a “grade III” placenta with significant calcification.

Image source: http://www.fetalultrasound.com/online/text/3-065.HTM
So while calcification of a placenta at term – around 39-42 weeks is part of the normal appearance of a full-term placenta and has no clinical significance in a healthy pregnancy, the appearance of significant calcification earlier in pregnancy is associated with risks to both the mother and baby. Just like we would be concerned about a very young person with wrinkles – it could be a sign of something significant happening.
Although, most every study has shown that calcification at term is normal and doesn’t mean anything in terms of negative outcomes for mum or baby, over the years, there has been conflicting evidence that early calcification was or wasn’t associated with poorer outcomes. That was because there were too many variables. In some studies, the mothers were smokers, which is associated with more calcification and more preterm births. In other studies, the mothers had hypertension, which can affect the health of the placenta and the baby. The studies were making comparisons on different ultrasound machines with interpretation by different technicians.
In a study of over 1000 pregnancies that controlled for these variables (Chen, Chen, & Lee, 2011), the participants agreed to frequent ultrasounds to monitor the development and progression of their baby’s placenta. The results indicated that when the placenta prematurely developed into a “grade III” with calcification prior to 32 weeks gestation, then,
The mother experienced increased
placental abruption
postpartum haemorrhage
transfer to the ICU
The baby experienced increased
preterm birth
low birth weight
low Apgar scores at 5 minutes (below 7)
neonatal death
However, if the placenta graduated to a “grade III” with calcification after 32 weeks gestation, then there were no increases in adverse outcomes. This was true whether the mother had other risk factors such as diabetes, hypertension, or smoking (Chen, Chen, & Lee, 2012).
Infarcts
Now let’s talk about those signs of “calcification” after the baby is born. Some placentas arrive with granular bumps across the maternal side and some parents are told that it’s a sign that the placenta was aging and starting to lose function. However, that’s not true for healthy full-term pregnancies.
Those granular bumps are not calcium deposits, but rather infarcts, deposits of fibrin, which are bits of scar tissue that have formed over dead cells through the process of infarction. Fibrin appears as small yellowish-white deposits that are the result of interference in the blood supply to the placenta.

Image source: http://wonderfullymadebelliesandbabies.blogspot.com/2012/11/variations-placentas-and-cords.html
Small placental infarctions (bumps of fibrin) are common in healthy full-term pregnancies and have no clinical significance. Only when there’s extensive infarction, meaning 10% or more of the placenta has died and been replaced by scar tissue is there an association with fetal growth restriction, fetal hypoxia, and fetal death, particularly if the infarctions occurred in the second and early third trimester (Mousa & Alfirevic1, 2000).
Infarcts can form at any point in the pregnancy and are associated with (Becroft, Thompson, & Mitchell, 2002; Naeye, 1977; Vinnars, Nasiell, Ghazi, Westgren, & Papadogiannakis, 2011):
maternal hyptertension
smoking
haemoglobin above 120, indicating poor blood volume expansion
maternal under-nutrition
So, in essence, when a mother is healthy and full term, calcification and infarcts are normal features of a healthy placenta – just like your healthy mother has some wrinkles and a few grey hairs.
This is one more bit of misinformation, mis-education, or pure nonsense that needlessly frightens healthy mothers into risky inductions.
Make wise choices, my friends.
Much love,
Mother Billie
References
Becroft, D. M. O., Thompson, J. M. D., & Mitchell, E. A. (2002). The epidemiology of placental infarction at term. Placenta, 23(4), 343-351.
Chen, K. H., Chen, L. R., & Lee, Y. H. (2011). Exploring the relationship between preterm placental calcification and adverse maternal and fetal outcome. Ultrasound in Obstetrics & Gynecology, 37(3), 328-334.
Chen, K. H., Chen, L. R., & Lee, Y. H. (2012). The role of preterm placental calcification in high-risk pregnancy as a predictor of poor uteroplacental blood flow and adverse pregnancy outcome. Ultrasound in medicine & biology, 38(6), 1011-1018.
Harris, R. D., & Alexander, R. D. (2000). Ultrasound of the placenta and umbilical cord. Ultrasonography in obstetrics and gynecology, 4, 597-625.
Jamal, A., Moshfeghi, M., Moshfeghi, S., Mohammadi, N., Zarean, E., & Jahangiri, N. (2017). Is preterm placental calcification related to adverse maternal and foetal outcome?. Journal of Obstetrics and Gynaecology, 37(5), 605-609.
Mousa, H. A., & Alfirevic1, Z. (2000). Do placental lesions reflect thrombophilia state in women with adverse pregnancy outcome?. Human Reproduction, 15(8), 1830-1833.
Naeye, R. L. (1977). Placental infarction leading to fetal or neonatal death. A prospective study. Obstetrics and gynecology, 50(5), 583-588.
Nolan, R. L. (1998). The placenta, membranes, umbilical cord, and amniotic fluid. A practical guide to ultrasound in obstetrics and gynecology, 438-439.
Vinnars, M. T., Nasiell, J., Ghazi, S. A. M., Westgren, M., & Papadogiannakis, N. (2011). The severity of clinical manifestations in preeclampsia correlates with the amount of placental infarction. Acta obstetricia et gynecologica Scandinavica, 90(1), 19-25.
Hocus Pocus - The ARRIVE study says inductions reduce caesareans
In an epic sleight of hand, the US obstetrical industry has managed to produce a study that affirms the “benefits” of universal elective induction of labour at 39 weeks. Headlines have trumpeted this remarkable accomplishment! Inducing labour early “prevents” c-sections!
The conclusion of the much anticipated ARRIVE study are presented in their abstract:
“IOL (induction of labour) in low-risk nulliparous women (first-time mothers) results in a lower frequency of CD (caesarean delivery) without a statistically significant change in the frequency of a composite of adverse perinatal outcomes.”
Obstetricians now have the much-desired go-ahead to routinely induce healthy first-time mothers prior to reaching 40 weeks under the guise that it will reduce c-sections with no additional negative outcomes to the mother or baby.
This is the same outrageous chicanery that brought us the ridiculously executed Term Breech Trial that changed obstetrical practices around the world. It was the excuse the industry was looking for to do what they already wanted to do: surgery.

In an epic sleight of hand, the US obstetrical industry has managed to produce a study that affirms the “benefits” of universal elective induction of labour at 39 weeks. Headlines have trumpeted this remarkable accomplishment! Inducing labour early “prevents” c-sections!
The conclusion of the much anticipated ARRIVE study (Grobman et al., 2018) are presented in their abstract:
“IOL (induction of labour) in low-risk nulliparous women (first-time mothers) results in a lower frequency of CD (caesarean delivery) without a statistically significant change in the frequency of a composite of adverse perinatal outcomes.”
Obstetricians now have the much-desired go-ahead to routinely induce healthy first-time mothers prior to reaching 40 weeks under the guise that it will reduce c-sections with no additional negative outcomes to the mother or baby.
This is the same outrageous chicanery that brought us the ridiculously executed Term Breech Trial that changed obstetrical practices around the world (Hannah et al., 2000). It was the excuse the industry was looking for to do what they already wanted to do: surgery (Hunter, 2013).
Obstetrics is a surgical speciality that also includes attending normal physiologic births. Years ago, the World Health Organisation sought to address disparities in health outcomes around the world in an effort to reduce maternal deaths in vulnerable places. They looked at countries with good outcomes and compared them to countries with poor outcomes. In wealthy nations where infrastructure was in place, food was easily accessible, and infection control measures were widely used, they tended to have a c-section rate around 5%. The WHO initially suggested that a c-section rate of 5-10% across the entire population could improve maternal-fetal outcomes. However, when the c-section rate rose above 15% across a population, the maternal death rate began to rise due to too much surgery.
There was naturally an outcry from the wealthy sector that was safely performing a lot of surgery and the WHO was roundly chastised for trying to prevent them from performing surgery on clients whom they believed would benefit from surgery. So the WHO said a c-section rate of 10-15% was “ideal” as it could potentially save lives, although they’ve subsequently stated that there is no benefit when the rate rises about 10% for a population (Betran, Torloni, et al, 2016).

Caesarean rates by country. (Betran, Ye, et al, 2016)
The problem wasn’t lack of surgery. The problem was that 99% of maternal deaths are in the developing world with half in sub-Sahara Africa and one-third in Southeast Asia where most fatal complications develop during pregnancy and are largely preventable or treatable. Half of these maternal deaths occur in fragile and humanitarian settings such as refugee displacement, natural disasters, and war (WHO, 2018).
Since the WHO’s mistake in encouraging an increase in surgery in impoverished, fragile, and humanitarian settings, the rest of the world’s obstetrics industry has spiraled out of control. Canada’s national c-section rate has risen to 28.2% in 2016-17 (CIHI, 2018) along with an increase in most every other country.
Data from around the world shows an average annual rate of increase in caesarean surgery of 4.4% from 1990 to 2014 (Betran, Ye, et al, 2016). Globally, in 2015 21.1% of all births occur through caesarean surgery, representing just over one in five mothers around the world (Boerma et al., 2018). This rate has risen from 12.1% of all births in 2000, representing a relative increase of 74.38% in just 15 years.
Regionally, caesarean rates are:
Latin America & Caribbean: 44.3% - an absolute increase of 19.4% and a relative increase of 77.91% (from 24.9% to 44.3%)
North America: 32.3% - an absolute increase of 10% and a relative increase of 44.84% (from 22.3% - 32.3%)
Oceania: 32.6% - an absolute increase of 14.1% and a relative increase of 76.22% (from 18.5% to 32.6%)
Europe: 27.3% - an absolute increase of 16.1% and a relative increase of 143.75% (from 11.2% to 27.3%)
Asia: 19.2% - an absolute increase of 15.1% and a relative increase of 343.18% (from 4.4% to 19.5%)
Africa: 7.3% - an absolute increase of 4.5% and a relative increase of 155.17% (from 2.9% to 7.4%)

Global increase in caesarean surgery 1990-2014. (Betran, Ye, et al, 2016)
What’s to blame for these shocking numbers? While it’s common to say it’s due to older, heavier, or more unhealthy mothers, the truth is that caesarean surgery has risen for every clientele group including young, slim, and healthy mothers.
The real increase in surgery comes from:
The management style of the hospital, where proactive management of patient flow and nursing resources results in more surgery and more postpartum haemorrhages (Plough et al., 2017)
Fear of litigation, particularly when malpractice premiums rise about $100,000 (Zwecker, Azoulay, & Abenhaim, 2011)
Financial incentives. Private facilities tend to perform more surgery as their clients have private insurance to pay for it (Dahlen et al., 2012). Even in the Canadian system, where compensation comes from a single payer through universal coverage, when the compensation for surgery is double that of a vaginal delivery, then there is a corresponding 5.6% increase in surgery when all else is equal (Allin, Baker, Isabelle, & Stabile, 2015)
Training, scheduling, and institutional culture drive the rates of surgery in individual institutions (Roth & Henley, 2012)
Both maternal request and maternal morbidity has been blamed for the dramatic increase in surgery, but neither has held up to scrutiny. The increase is physician induced (Roth & Henley, 2012).

Tomasz Kobosz freeimages.com
Now this same industry that has brought us shockingly high rates of surgery due to the nature of the industry says they have a “solution” for this epidemic: induce healthy mothers early.
The caesarean epidemic is due to the industry wanting to perform surgery. The unsupportable conclusions of the Term Breech Trial turned the industry upside-down in a heartbeat and most mothers with a breech-presenting baby are now faced with mandatory surgery. This industry is so invested in getting their way that some of their members have even resorted to using the courts to force clients into non-consenting procedures (Diaz-Tello, 2016).
The idea that inducing a mother early will reduce the incidence of caesarean surgery is akin to saying that if you give a child a pre-dinner snack then they are less likely to over-eat at dinner. Fulfilling the need to medically manage the client’s physiology satisfies the surgeon’s training, preferences, and institutional culture that guide the physician to perform surgery. This is nothing more than a physician placebo. And when this pre-dinner snack doesn’t satisfy any more, and the honeymoon phase of routine early induction wanes, then rates of surgery will rebound.
To begin, an induction is not benign. The risks associated with an induction depend on what is done to the patient. This could involve multiple vaginal exams (infection, sexual re-traumatisation), artificial rupture of membranes (cord prolapse, infection, foetal distress), continuous foetal monitoring (caesarean surgery), chemical cervical ripening (uterine hyperstimulation, uterine rupture, foetal distress, maternal death, foetal death, meconium), IV synthetic oxytocin (Pitocin/syntocinon) (uterine rupture, postpartum haemorrhage, breastfeeding failure, postpartum depression and anxiety, water intoxication leading to convulsions, coma or death, foetal distress, meconium, neonatal jaundice, neonatal brain damage, and neurological dysregulation in the child years later) (Gregory, Anthopolos, Osgood, Grotegut, & Miranda, 2013; Grotegut, Paglia, Johnson, Thames, & James, 2011; Gu et al., 2016; Kurth & Haussmann, 2011; Elkamil et al., 2011).
Inductions are generally more painful and first time mothers are more than 3x more likely to ask for an epidural during an induction (Selo-Ojeme et al., 2011). This leads to a longer labour and pushing stage, need for more synthetic oxytocin, problems passing urine, inability to move after the birth, fever, and more instrumental deliveries (Anim-Somuah, Smyth, Cyna, & Cuthbert, 2018).
Now let’s talk about the study itself.
A total of 3062 women were assigned to labour induction, and 3044 were assigned to expectant management (wait and see approach). Just like with the Term Breech Trial, there was quite a bit of crossover, meaning those who were assigned to the induction group had a spontaneous birth and those who were assigned to a wait-and-see approach were induced (about 5% from each group – 1 in 20 participants). However, the results were reported to the group they were assigned to.
The enrolment was designed to be too small to detect certain outcomes. Adverse outcomes such as maternal death, cardiac arrest, anaesthetic complications, thromboembolism, amniotic fluid embolism, major puerperal infection, or haemorrhage are fairly rare but are associated with both induction and surgery.
Without enough participants, it’s not possible to determine if there was an increase in adverse outcomes from inducing mothers.
Remember, this study took place in the US where they boast some of the worst maternal and neonatal outcomes in the developed world. How they practice obstetrics has much to do with this. Both the induction and the expectant management groups experienced high rates of interventions and the outcomes for the babies were consistent with that:
15% were not breathing at all or were breathing weakly 5 minutes after birth
12% were admitted to the NICU
5% had neonatal jaundice
1% needed breathing support for a day or more
0.7% experienced meconium aspiration syndrome
0.6% had hypoxic ischemic encephalopathy
0.3% suffered intracranial haemorrhage
0.3% had infections
0.2% had seizures
The results for the mothers were equally awful:
5% had severe postpartum haemorrhage of over 1500cc requiring a blood transfusion, blood products, or a hysterectomy
4% suffered a third or fourth degree perineal tear
2% had a postpartum infection

Benjamin Earwicker freeimages.com
With shockingly terrible results like this, the industry has the temerity to suggest that signing up for an elective induction to placate their nerves is a good idea because they’re less likely to perform surgery?
Frankly, it’s asinine nonsense from a group that needs a dramatic change in education and culture. We’ll see how long it takes for this insanity to move throughout the obstetrical world.
Make wise choices, my friends.
Much love,
Mother Billie
References
Allin, S., Baker, M., Isabelle, M., & Stabile, M. (2015). Physician Incentives and the Rise in C-sections: Evidence from Canada (No. w21022). National Bureau of Economic Research.
Anim-Somuah, M., Smyth, R. M., Cyna, A. M., & Cuthbert, A. (2018). Epidural versus non-epidural or no analgesia for pain management in labour. The Cochrane database of systematic reviews, 5, CD000331-CD000331.
Betrán, A. P., Torloni, M. R., Zhang, J. J., Gülmezoglu, A. M., WHO Working Group on Caesarean Section, Aleem, H. A., ... & Deneux‐Tharaux, C. (2016). WHO Statement on caesarean section rates. BJOG: An International Journal of Obstetrics & Gynaecology, 123(5), 667-670.
Betrán, A. P., Ye, J., Moller, A. B., Zhang, J., Gülmezoglu, A. M., & Torloni, M. R. (2016). The increasing trend in caesarean section rates: global, regional and national estimates: 1990-2014. PloS one, 11(2), e0148343.
Boerma, T., Ronsmans, C., Melesse, D., Barros, A., Barros, F., Juan, L., Moller, A., Say, L., Hosseinpoor, A., Mu, Y., Neto., D., Temmerman, M. (2018). Global epidemiology and use of and disparities in caesarean section. The Lancet. Volume 392, Issue 10155, P1341-1348, October 12, 2018.
CIHI. Canadian Institute for Health Information. (2018). Hospital Morbidity Database, 2016–2017.
Dahlen, H. G., Tracy, S., Tracy, M., Bisits, A., Brown, C., & Thornton, C. (2012). Rates of obstetric intervention among low-risk women giving birth in private and public hospitals in NSW: a population-based descriptive study. BMJ open, 2(5), e001723.
Diaz-Tello, F. (2016). Invisible wounds: obstetric violence in the United States. Reproductive Health Matters.
Elkamil, A. I., Andersen, G. L., Salvesen, K. Å., Skranes, J., Irgens, L. M., & Vik, T. (2011). Induction of labor and cerebral palsy: a population‐based study in Norway. Acta obstetricia et gynecologica Scandinavica, 90(1), 83-91.
Gommers, J. S., Diederen, M., Wilkinson, C., Turnbull, D., & Mol, B. W. (2017). Risk of maternal, fetal and neonatal complications associated with the use of the transcervical balloon catheter in induction of labour: A systematic review. European Journal of Obstetrics & Gynecology and Reproductive Biology, 218, 73-84.
Gregory, S. G., Anthopolos, R., Osgood, C. E., Grotegut, C. A., & Miranda, M. L. (2013). Association of autism with induced or augmented childbirth in North Carolina Birth Record (1990-1998) and Education Research (1997-2007) databases. JAMA pediatrics, 167(10), 959-966.
Grotegut, C. A., Paglia, M. J., Johnson, L. N., Thames, B., & James, A. H. (2011). Oxytocin exposure during labor among women with postpartum hemorrhage secondary to uterine atony. American journal of obstetrics and gynecology, 204(1), 56-e1.
Grobman, W. A., Rice, M. M., Reddy, U. M., Tita, A. T., Silver, R. M., Mallett, G., ... & Rouse, D. J. (2018). Labor induction versus expectant management in low-risk nulliparous women. New England Journal of Medicine, 379(6), 513-523.
Gu, V., Feeley, N., Gold, I., Hayton, B., Robins, S., Mackinnon, A., ... & Zelkowitz, P. (2016). Intrapartum synthetic oxytocin and its effects on maternal well‐being at 2 months postpartum. Birth, 43(1), 28-35.
Hannah, M. E., Hannah, W. J., Hewson, S. A., Hodnett, E. D., Saigal, S., Willan, A. R., & Collaborative, T. B. T. (2000). Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. The Lancet, 356(9239), 1375-1383.
Hunter, B. (2013). Implementing research evidence into practice: some reflections on the challenges. Evidence based midwifery, 11(3), 76-80.
Kurth, L., & Haussmann, R. (2011). Perinatal Pitocin as an early ADHD biomarker: neurodevelopmental risk?. Journal of attention disorders, 15(5), 423-431.
Linton, A., Peterson, M. R., & Williams, T. V. (2004). Effects of maternal characteristics on cesarean delivery rates among US Department of Defense healthcare beneficiaries, 1996–2002. Birth, 31(1), 3-11.
Plough, A. C., Galvin, G., Li, Z., Lipsitz, S. R., Alidina, S., Henrich, N. J., ... & McDonald, R. (2017). Relationship between labor and delivery unit management practices and maternal outcomes. Obstetrics & Gynecology, 130(2), 358-365.
Roth, L. M., & Henley, M. M. (2012). Unequal motherhood: racial-ethnic and socioeconomic disparities in cesarean sections in the United States. Social Problems, 59(2), 207-227.
Selo-Ojeme, D., Rogers, C., Mohanty, A., Zaidi, N., Villar, R., & Shangaris, P. (2011). Is induced labour in the nullipara associated with more maternal and perinatal morbidity?. Archives of gynecology and obstetrics, 284(2), 337-341.
Washington, S., Caughey, A. B., Cheng, Y. W., & Bryant, A. S. (2012). Racial and ethnic differences in indication for primary cesarean delivery at term: experience at one US Institution. Birth, 39(2), 128-134.
WHO, World Health Organization. (2018). Fact Sheet-Maternal Mortality.
Zwecker, P., Azoulay, L., & Abenhaim, H. A. (2011). Effect of fear of litigation on obstetric care: a nationwide analysis on obstetric practice. American journal of perinatology, 28(04), 277-284.
The Textbook is Wrong
We were sitting across her kitchen table. A tissue was being nervously mangled in her trembling hands.
“I just can’t do it again,” she said. “Can you tell me about your daughter’s birth,” I asked her?
She explained that everyone told her it was a good birth. Her doctor said it was textbook perfect. Her mother was there and repeated her version of her granddaughter’s birth to everyone who would listen. It was natural. It was quick. It was the best day ever.
And as the story unfolded, tears welled up in my eyes, finally spilling down my own cheeks. It was an awful experience. And my heart broke into pieces again.
She described a birth where she was tortured with screamingly painful vaginal exams, weeping for them to stop, thrashing to escape the confines of the hospital bed where she was tethered to the monitoring machine for policy’s sake, begging to stand up, move, sway, anything to cope with her rapidly advancing labour. Her voice buried under a gentle shush so as not to scare the other mothers.
We were sitting across her kitchen table. A tissue was being nervously mangled in her trembling hands.
“I just can’t do it again,” she said. “Can you tell me about your daughter’s birth,” I asked her?
She explained that everyone told her it was a good birth. Her doctor said it was textbook perfect. Her mother was there and repeated her version of her granddaughter’s birth to everyone who would listen. It was natural. It was quick. It was the best day ever.
And as the story unfolded, tears welled up in my eyes, finally spilling down my own cheeks. It was an awful experience. And my heart broke into pieces again.
She described a birth where she was tortured with screamingly painful vaginal exams, weeping for them to stop, thrashing to escape the confines of the hospital bed where she was tethered to the monitoring machine for policy’s sake, begging to stand up, move, sway, anything to cope with her rapidly advancing labour. Her voice buried under a gentle shush so as not to scare the other mothers.

When the baby emerged, she was placed on her mother as the room cheered. Only, she felt nothing. Grateful that those hands wouldn’t enter her again, except in her dreams. The symptoms of PTSD followed her for the first year of her child’s life as she struggled to connect the version of her birth she’d been told and her personal experience of it.
And she just couldn’t do it again.
This is the story I hear over and over by mothers in all parts of the world. She’s told to be grateful for her healthy baby, to be grateful for the care she received, that her expectations were too high, that having a baby is hard and she had a low pain threshold, or that she was foolish for not taking the drugs offered her. She’s told anything except, “I’m sorry. It wasn’t meant to be that way.”
Research tells us that trauma is not particularly related to any emergencies or complications, but is dependent on how the mother experiences her birth. What can seem like a “textbook” birth to the clinician can be a devastating experience for the mother.
Birth is a hormonal process driven by our para-sympathetic nervous system, our “calm and connected” system. The primary driver of birth is oxytocin, which is the hormone of love, trust and bonding. Endorphins and prolactin ensure the experience is filled with pain-relief and joy. In today’s culture of fear, mothers are increasingly experiencing their births as traumatic as hospital policies serve the business end of cost-control, expediency, and insurance regulations. Doctors, nurses and midwives are sometimes constrained by policy in spite of the best interests of their clients.
Where birth is biologically programmed to be joyous, active, patient and primed for love and bonding, how we do birth in this culture is at odds with this biological imperative. The problem comes from what we call “textbook perfect”. The textbook is written from a medicalised perspective that is brand new in the biology of humans. Humans haven’t yet adapted to forced fasting, routine IVs, ultrasounds, continuous monitoring, hospital acquired infections, vaginal penetrations, forced on-her-back pushing, an inability to move and strangers between her legs.
When one third of mothers say their births were traumatic and one in ten struggle with PTSD, we know that birth is in crisis. And the textbook is wrong.
Of course, some births require medical assistance. Yet the question becomes, how can we protect a mother from trauma? And what happens when a pregnant mother says she can’t do that again?

In spite of the law that says a medical procedure cannot be performed on a non-consenting patient and that consent may be withdrawn at any point for any reason, the truth is that many things happen to a mother in labour in which she has no choice. In order to gain compliance, she may be told the baby might die. We call this ‘playing the dead baby card’ and it’s so common it’s becoming a laughing point.
There have been many a new textbooks written – from the mother’s perspective, from the baby’s perspective, from the vantage of good science, and yet mothers are still struggling. When a mother says she can’t do it again, it means we have to take a long hard look at what is happening today.
Strong and courageous leadership from medical associations including obstetricians, family physicians, nurses and midwives could lead the way in changing non-evidence based policies that serve the institution and insurance regulations but harm mothers and babies.
Mothers are increasingly learning the science of safe birth for themselves and are changing the conditions under which they give birth. Perhaps the quickest route to change is to spend our birthing dollars in those places that support the biology of birth and the law of informed consent and refusal.
It’s not selfish to want a great experience – it’s biology.