
Gestational diabetes rises 300% since Australia added folic acid to the food supply.
This research rant was triggered by a recent study, Maternal Folate Excess, Placental Hormones, and Gestational Diabetes Mellitus: Findings from Prospective Cohorts Before and After Mandatory Folic Acid Food Fortification (2025) which showed that since Australia’s mandatory fortification of bread flour in 2009 with synthetic folic acid, there’s been a tripling of the incidence of gestational diabetes. They suggest that folic acid has a negative effect on placental hormones that regulate insulin sensitivity. While the diagnosis of gestational diabetes has increased since the WHO changed its diagnostic criteria, it doesn’t account for the whopping increase seen since mandatory fortification. “A combination of FA (folic acid) food fortification, both mandatory and voluntary, increased dose of supplementation and continued supplementation beyond the recommended first trimester, have resulted in maternal folate excess, levels that far exceed the established clinical reference range.”
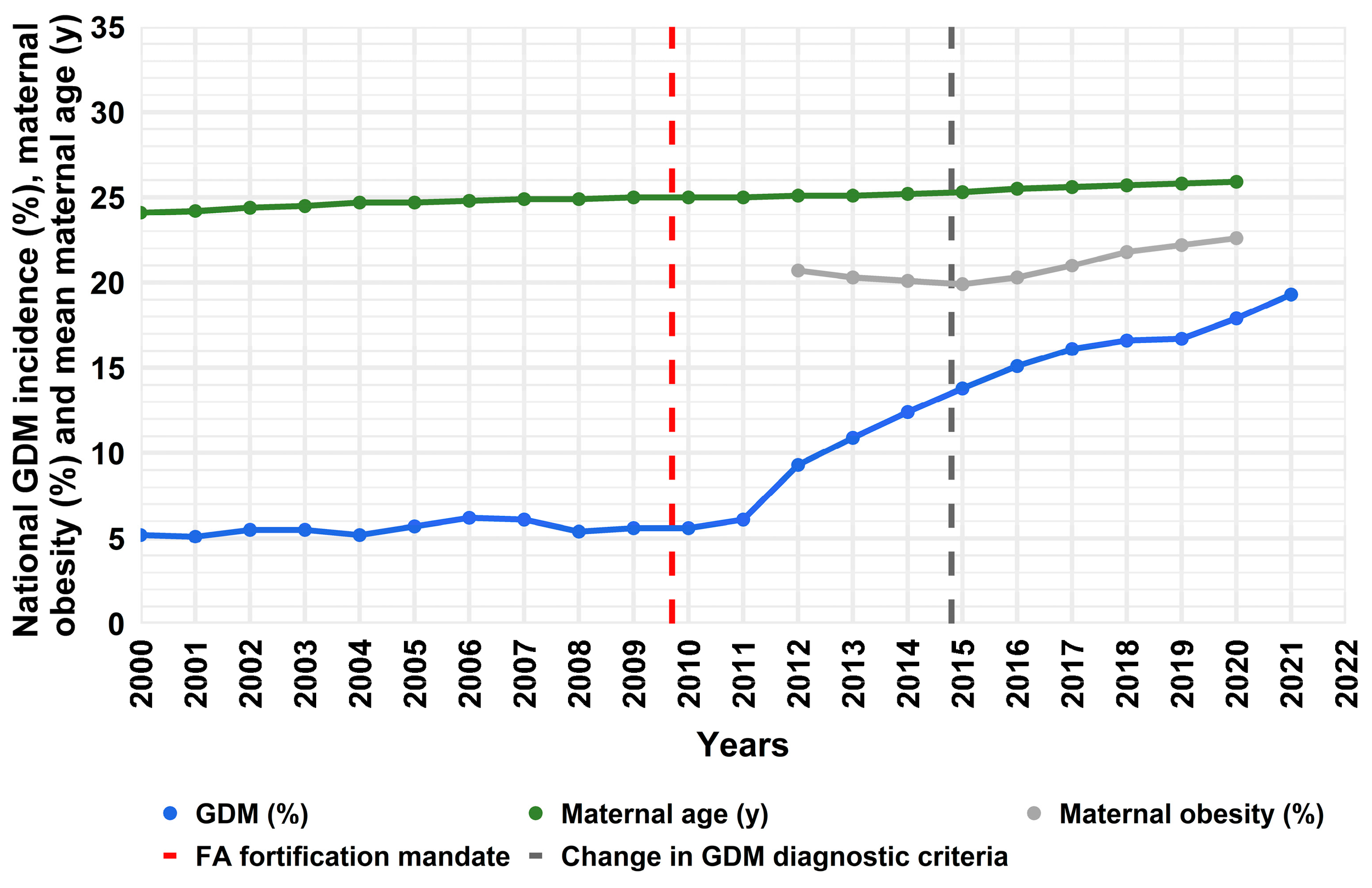
Figure 1. Incidence of GDM, maternal age and obesity in Australia (AIHW trends over time data) [1]. National GDM incidence is indicated by the solid blue line; Mean national maternal age is shown in green; National maternal obesity data (grey) is incomplete prior to 2012; Dashed vertical lines indicate implementation of FA food fortification mandate (red) and the change in WHO diagnostic criteria (dark grey).
In the middle of the last century, modern living moved away from traditionally prepared whole foods for the convenience of processed foods. These processed foods lacked their original nutrients resulting in population-wide deficiencies in B vitamins and iron. The solution was to add back in a few missing elements to processed wheat flour and other grains (depending on country). Folate was added to this fortification mandate a little later in 1998 in the US & Canada with the synthetic form of folate, folic acid, which is cheap and shelf stable.
The specific purpose of mandatory fortification with folic acid was to reduce the incidence of neural tube defects in developing embryos, which is associated with folate deficiency. While the woman about to conceive was targeted for this intervention, everyone who consumed flour-based products were on the receiving end.
The neural tube is a structure that develops into the brain, spinal cord, and surrounding protective tissues. When it fails to close during early embryonic development, that is, within the first 4 weeks after conception, some parts of the baby’s spinal column or brain may remain open. The most common form is spina bifida which can often be surgically closed after birth. Anencephaly is more severe where parts of the brain or skull fail to develop most often resulting in stillbirth or death shortly after birth.
Health agencies recommend that women planning to conceive supplement with 400 μg of folic acid preconception and for the first 12 weeks of pregnancy, although that exceeds the time the baby’s neural tube is closing. Since many pregnancies are unplanned, women of childbearing age are encouraged to routinely supplement with folic acid. Most prenatal vitamins will contain the recommended 400 μg whereas some will have significantly more.
While this all seems terrific, there are significant concerns with medicating our food supply with a synthetic vitamin and suggesting further supplementation for pregnant women.
Worldwide data suggests that folic acid fortification in the food supply is associated with a 50%-100% increase in mean plasma folate across the population with a 25%-50% reduction in neural tube defects compared to countries with no fortification. (Quinn et al., 2024)
There is evidence that actual amounts of folic acid in our food supply exceeds what was originally intended to the tune of 115%-188% of the intended value. (Shakur et al., 2009)
A systematic review (Ledowski et al., 2022) found that almost all women who were taking a folic acid supplement exceeded the recommended upper limit of 1000 μg per day.
As a synthetic compound, folic acid is metabolised differently than naturally occurring folate as found in food. Folic acid requires a two-step reduction in order to become biologically available. This reduction occurs mostly in the liver, however, most tissues, including the liver, have a limited ability to reduce folic acid due to low activity of an enzyme called DHFR. Further, the process of absorbing and transforming folic acid into its active form (5-methyltetrahydrofolate) becomes saturated around >200–400 μg of folic acid. This means unmetabolised folic acid is left to circulate in the bloodstream. (Patel and Sobczyńska-Malefora, 2016)
In fact, nearly all blood samples from US children and adults show unmetabolised folic acid since the medication of their food supply. (Pfeiffer et al., 2015)
As outlined in a review by Patel and Sobczyńska-Malefora (2016), high levels of circulating folic acid have been linked to increased cancer risk and increased progression of cancer for certain groups due to its ability to enhance cell replication and reduce natural killer cell response to cancerous cells. It can mask a B12 deficiency and is toxic to the liver at high concentrations.
In pregnancy, high levels of folic acid have been linked to insulin resistance and greater fat stores in children and may be contributing to increasing childhood obesity and type 2 diabetes.
In women with a DHFR gene mutation (about 20% of the US population) their babies were more likely to develop retinoblastoma, a rare cancer of the eye. Further, those with this particular gene mutation are more susceptible to the effects of folic acid in the form of impaired memory and cognition.
Based on animal studies, supplemental folic acid during pregnancy may increase the incidence of epilepsy in the baby.
Excess circulating folic acid in pregnancy is also associated with tongue ties in the baby. (Kesuma et al., 2025)
The medication of our food supply in lieu of education on nutrition and better availability of wholesome foods, along with aggressive supplementation recommendations, may have contributed to the explosion of cancers, obesity, diabetes, and other health consequences seen in the last 25+ years.
Adequate folate is needed for human functioning and for the proper development of precious new humans. While we can’t unmedicate our food, we can choose other sources of folate and use supplements cautiously.